Biomicroscopy of the cornea. Biomicroscopy
The eyes are the most important sense organ. With its help, a person perceives 70% of information coming from outside. The matter concerns not just the formation of images, but also adaptation to the terrain, reducing the risk of injury, and the organization of social life.
Therefore, when the eyes are affected due to injury, age-related changes or general diseases, the question is about disability and a noticeable decrease in the quality of life. It is for the purpose of early and accurate diagnosis of diseases of the organ of vision in ophthalmology that there is a quick and informative method biomicroscopy.
What is the biomicroscopy method?
Biomicroscopy - microscopic examination of structures visual organ in vivo (in a living organism) using a slit lamp (biomicroscope).
Slit lamp - optical instrument, consisting of:
- Binocular (for two eyes) microscope - a device for obtaining images magnified up to 60 times.
- Light source: halogen or LED lamps with a power of 25W.
- Slit diaphragm - to create thin vertical or horizontal beams of light.
- Supports for the patient's face (support under the chin and forehead).
- Aspheric Grud lens - for biomicroophthalmoscopy (examination of the fundus using a slit lamp).
The image acquisition method is based on the optical Tyndall effect. A thin beam of light is passed through an optically inhomogeneous medium (cornea - lens - vitreous body). The examination is carried out perpendicular to the direction of the rays. The resulting image appears in the form of a thin, cloudy light strip, the analysis of which is the conclusion of biomicroscopy.
Types of biomicroscopy
Examination of the eyes using a slit lamp is a standard technique, but there are different methods illumination of the biomicroscope is described below.
- Diffuse lighting. Most often this method is used as initial stage research. With its help, at a slight magnification, a general examination of the structures of the eye is carried out.
- Direct focal illumination. The most used method, since it provides the opportunity to examine all the superficial structures of the eye: cornea, iris, lens. When directing the light beam, a wider area is first illuminated, then the aperture is narrowed for a more detailed study. The method is useful for early diagnosis keratitis (inflammatory process in the cornea) and cataracts (clouding of the lens).
- Indirect focal illumination (dark field examination). The doctor's attention is drawn to areas located next to the illuminated area. Under such conditions, empty vessels, folds of Descemet's membrane, and small precipitates (sedimentary complexes) are clearly visualized. In addition, the method is used for the differential diagnosis of iris tumors.
- Variable (oscillatory) lighting is a method that combines the previous two methods. With a rapid change of bright light and darkness, the reaction of the pupil is studied, as well as small foreign bodies, which in such conditions give a characteristic shine.
- Mirror field method: a study of reflective zones is carried out. Technically, this method is considered the most difficult, but its use makes it possible to identify the smallest changes in the surface of the eye structures.
- Transmitted (reflected) lighting. The elements are studied through a beam of light reflected from another structure (for example, the iris in light reflected from the lens). The value of the method lies in the study of structures that are inaccessible under other lighting conditions. In reflected light, thin scars and swelling of the cornea, thinning of the pigment layers of the iris, and small cysts under the anterior and posterior capsules of the lens are visible.
Important! When examining the structures of the eye in reflected light, the areas under study acquire the color of the structures from which the light beam came. For example, when light is reflected from a blue iris, the lens under study acquires a gray-blue color
Due to widespread use ultrasound diagnostic methods appeared new option research - ultrasound biomicroscopy. It can be used to identify pathological changes in the lateral parts of the lens, on the posterior surface of the iris and in the ciliary body.
Indications for the study
Taking into account the capabilities of the method and the wide field of view, the list of indications for biomicroscopy is quite large:
- Conjunctivitis (inflammation of the conjunctiva).
- Pathologies of the cornea: erosions, keratitis (inflammation of the cornea).
- Foreign body.
- Cataract (clouding of the lens).
- Glaucoma (a condition characterized by increased intraocular pressure).
- Anomalies in the development of the iris.
- Neoplasms (cysts and tumors).
- Dystrophic changes in the lens and cornea.
The additional use of a Grud lens makes it possible to diagnose pathologies of the retina, optic nerve head and vessels located in the fundus.
Contraindications to biomicroscopy
There are no absolute contraindications for diagnostic manipulation. However, biomicroscopy is not performed on people with mental illness and patients under the influence of drugs or alcohol.
How the research works
Biomicroscopy does not require prior preparation of the patient.
Doctor's advice! Biomicroscopy is recommended for children under 3 years of age in a horizontal position or in a state of deep sleep.
The patient is examined in a dark room (for greater contrast between illuminated and darkened areas) of the ophthalmology office of a clinic or hospital.
Important! If you plan to examine the vitreous body and structures in the fundus, mydriatics are dripped immediately before the procedure ( medicines, dilating the pupils).
Fluorescein drops are used to detect violations of the integrity of the cornea
The patient sits in front of the slit lamp, places his chin on a special stand, and presses his forehead against the bar. It is recommended not to move during the examination and to blink as little as possible.
Using a control joystick, the doctor determines the size of the slit in the diaphragm and directs a beam of light to the area being examined. Using different lighting methods, all structures of the eye are examined. The duration of the procedure is 15 minutes.
Possible complications after biomicroscopy
Biomicroscopy does not cause discomfort or pain. The only undesirable consequence may be allergic reaction on the drugs used.
Important! If a foreign body is detected during the examination, before removing it, use eye drops Lidocaine. Therefore, you need to notify your doctor if you are allergic to the drug.
Advantages of the method
The ability to study the state of the superficial and deep structures of the visual organ makes biomicroscopy the method of choice for diagnosing most ophthalmological diseases. To objectively assess the benefits of this study, comparison with other diagnostic methods is necessary.
|
Criterion |
Biomicroscopy |
Ophthalmoscopy |
|
Invasiveness of the study |
Non-invasive, non-contact |
Non-invasive, non-contact |
|
Duration of the procedure |
10-15 minutes |
|
|
Structures studied |
|
|
|
Field width |
360 degrees |
270 degrees |
|
Image Resolution |
Depends on the vision of the ophthalmologist and the distance from which the examination is carried out |
|
|
Possibility of storing objective data |
On digital media |
Examination of the eye using a slit lamp and changing lighting allows you to see the smallest signs of pathologies of all structures. A separate advantage of the method is its low cost when using new biomicroscopes with aspherical lenses and tonometers, replacing traditional tonometry and ophthalmoscopy.
How to decipher the results of biomicroscopy

When examining a healthy eye, the following is determined:
- Cornea: convex-concave prism with a slight bluish glow. Nerves and blood vessels are visible in the thickness of the cornea.
- Iris: the pigment layer is represented by a colored (depending on the color of the eyes) fringe around the pupil, and in the ciliary zone zones of contraction of the ciliary muscle are visible.
- Lens: A transparent body that changes shape when focused. It consists of an embryonic nucleus covered with a cortex, anterior and posterior capsule.
Variants of possible pathologies and the corresponding biomicroscopic picture are presented in the table.
|
Disease |
Biomicroscopic picture |
|
Glaucoma |
|
|
Cataract |
|
|
Foreign body and eye injuries |
|
|
|
|
Coloboma of the iris (a congenital anomaly where part of the iris is missing) |
|
|
Eye tumors |
|
Due to its diagnostic value, ease of performance and safety, biomicroscopy has become a standard procedure for examining ophthalmic patients, along with measuring visual acuity and examining the fundus.
The video below describes the technique of biomicroscopy.
Examination of the internal structures of the eye is necessary when there is a suspicion of any diseases or anomalies of the anterior or posterior part eyeball. The use of a special microscope for this purpose, combined with a powerful lighting device, is called biomicroscopy. This study helps to identify and study in detail many abnormalities within the visual organ.
Biomicroscopy: basic concepts
Biomicroscopy is the examination of the internal state of the eyeball using a medical device called a slit lamp. Includes a wide range of complex imaging techniques for pathologies of varying origin, texture, color, transparency, size and depth.
The slit lamp allows for detailed microscopic examination of the eye
A slit lamp is an instrument consisting of a high-intensity light source that can be focused to direct a thin strip of light into the eye through various filters that provide the location and size of the slit. It is used in combination with a biomicroscope, which, together with the illuminator, is mounted on one coordinate table. The lamp facilitates inspection of the anterior and posterior segments of the human eye, which include:
- eyelid;
- sclera;
- conjunctiva;
- iris;
- natural lens (lens);
- cornea;
- vitreous body;
- retina and optic nerve.
The slit lamp is equipped with a diaphragm that forms a slit up to 14 mm in width and height. A binocular microscope includes two eyepieces and an objective (magnifying lens), the optical power of which can be adjusted using a dial that changes the magnification factor. The range of gradual increase is from 10 to 25 times. With an additional eyepiece - up to 50-70x.
Binocular slit lamp examination provides stereoscopic, magnified images of ocular structures in detail, allowing anatomical diagnoses to be made for a variety of ocular conditions. The second, hand-held lens is used to examine the retina.
For a full examination with a biomicroscope, there are various methods of slit lamp illumination. There are six types of basic lighting options:
- Diffuse illumination - examination through a wide aperture using glass or a diffuser as a filter. It is used for a general examination to detect the localization of pathological changes.
- Direct focal illumination is the most commonly used method, which consists of observing using an optical slit or direct focal illumination of rays. A thin or medium width slit is directed and focused on the cornea. This type of illumination is effective for determining the spatial depth of ocular structures.
- Specular reflection, or reflected lighting, is a phenomenon similar to the image visible on the sunny surface of a lake. Used to assess the endothelial contour of the cornea (its inner surface). To achieve a mirror effect, the tester directs a narrow beam of light to the eye from the temple side at an angle of about 25-30 degrees to the cornea. A bright area of specular reflection will be visible on the corneal epithelium (outer surface).
- Transillumination (transillumination), or examination in reflected (transmitted) light. In some cases, illumination with an optical slit does not provide sufficient information or is simply impossible. Transillumination is used to examine transparent or translucent structures - the lens, the cornea - by reflecting rays from deeper tissues. To do this, highlight the background of the object under study.
- Indirect lighting - a light beam passing through translucent fabrics is scattered, simultaneously highlighting individual places. Used to identify pathologies of the iris.
- Scleral scattering - with this type of lighting, a wide beam of light is directed at the limbal region of the cornea (the edge of the cornea, the junction with the sclera) at an angle of 90 degrees to it to create a light scattering effect. In this case, a certain halo appears under the cornea, which illuminates its anomalies from the inside.
The slit lamp makes it possible to study the structural parts of the cornea:
- epithelium;
- endothelium;
- posterior border plate;
- stroma.
And also - determine the thickness of the transparent outer shell, its blood supply, the presence of inflammation and edema, and other changes caused by injury or dystrophy. The study allows you to study in detail the condition of scars, if they exist: their size, adhesions with surrounding tissues. Biomicroscopy reveals tiny solid deposits on the back surface of the cornea.
If a corneal pathology is suspected, the doctor will additionally prescribe confocal microscopy - an assessment method morphological changes this organ using a special microscope with a magnification of 500 times. It allows you to study in detail the layer-by-layer structure of the corneal epithelium.
During biomicroscopy of the lens, the doctor examines the optical section for possible clouding of its substance. Determines the location pathological process, which often begins precisely at the periphery, the state of the nucleus and capsule. When examining the lens, almost any type of lighting can be used. But the most common are the first two: diffuse and direct focal lighting. They are usually carried out in this order. The first type of lighting allows you to evaluate the general appearance of the capsule and see foci of pathology, if any. But for a clearer understanding of where exactly the “breakdown” occurred, it is necessary to resort to direct focal lighting.
Examining the vitreous body using a slit lamp is a challenging task that not every novice in ophthalmology can handle. The vitreous body has a jelly-like consistency and lies quite deep. Therefore, it weakly reflects light rays.
Biomicroscopy of the vitreous body requires acquired skill
In addition, the study is hampered by a narrow pupil. An important condition High-quality biomicroscopy of the vitreous body is pre-medicated mydriasis (pupil dilation). The room where the inspection is carried out should be as dark as possible, and the area under study, on the contrary, should be quite brightly lit. This will provide the necessary contrast, since the vitreous body is a weakly refractive optical medium that slightly reflects light. The doctor uses mostly direct focal lighting. When examining the posterior parts of the vitreous body, it is possible to study in reflected light, where the fundus of the eye plays the role of a reflective screen.
Focusing light on the fundus allows one to examine the retina and optic nerve head in an optical section. Early detection of neuritis or swelling of the nerve (congestive papilla), retinal tears helps in the diagnosis of glaucoma, prevents optic nerve atrophy and decreased vision.
The slit lamp will also help determine the depth of the anterior chamber of the eye, detect cloudy changes in moisture and possible impurities of pus or blood.
A wide selection of lighting types thanks to special filters allows you to clearly study the vessels, detect areas of atrophy and tissue ruptures. Biomicroscopy of translucent and opaque tissues of the eyeball (for example, conjunctiva, iris) is less informative.
Slit lamp device: video
Indications and contraindications
Biomicroscopy is used to diagnose:
- glaucoma;
- cataracts;
- macular degeneration;
- retinal detachment;
- corneal damage;
- blockage of retinal vessels;
- inflammatory diseases;
- neoplasms, etc.
You can also detect an injury to the eye, foreign bodies in it, which x-rays cannot show.
There are no absolute contraindications for slit lamp examination. However, it is worth paying attention to some important nuances associated with eye injuries:

Observation of fundus known as fundus lens ophthalmoscopy. But with a slit lamp, direct observation of the bottom is impossible due to the refractive power of the ocular media, as a result of which the microscope does not provide focusing. The use of auxiliary optics helps. Using a diagnostic three-mirror Goldmann lens in the light of a slit lamp, you can examine those peripheral areas of the retina that cannot be examined with ophthalmoscopy.
Advantages and disadvantages of the method
Biomicroscopy has a number of significant advantages over other methods of ophthalmological examination:
- Possibility of precise localization of anomalies. Due to the fact that a beam of light from a slit lamp during biomicroscopy can penetrate into the structures of the eye from different angles, it is quite possible to determine the depth of pathological changes.
- Increased diagnostic capabilities. The device provides lighting in vertical and horizontal planes at different angles.
- Convenient for detailed inspection of a specific area. A narrow beam of light directed into the eye provides contrast between the illuminated and darkened areas, forming the so-called optical slice.
- Possibility of biomicroophthalmoscopy. The latter is successfully used for examining the fundus.
The method is considered highly informative, devoid of significant disadvantages and contraindications. But in some cases it is advisable to prefer a manual device to a stationary one, although a manual slit lamp has limited capabilities. For example, it is used:
- for biomicroscopy of the eyes of babies who are still in a supine position;
- when examining restless children who cannot sit for the prescribed amount of time at a conventional slit lamp;
- for examining patients in the postoperative period, during strict bed rest, it is an alternative to the stationary version of the device.
In these cases, a hand-held lamp has advantages over scattered (diffuse) lighting and makes it possible to examine in detail the surgical incision and the anterior chamber with intraocular fluid, the pupil, and the iris.
The manual slit lamp has modest capabilities, but sometimes it is indispensable
Carrying out the procedure
The examination is carried out in a darkened room. The patient sits in a chair, places his chin and forehead on a support to fix his head. She must be motionless. It is advisable to blink as little as possible. Using a slit lamp, the ophthalmologist examines the patient's eyes. To aid the examination, a thin strip of paper containing fluorescein (a glowing dye) is sometimes applied to the edge of the eye. This colors the tear film on the surface of the eye. The paint is later washed away by tears.
Then, at the doctor's discretion, drops may be needed to dilate the pupils. You must wait 15 to 20 minutes for the medicine to take effect, after which the examination is repeated, which allows you to check back eyes.
Sometimes before biomicroscopy it is necessary to dilate the pupil with medication
First, the ophthalmologist will again test the anterior structures of the eye, and then, using a different lens, examine the back of the organ of vision.
As a rule, such a test does not cause significant side effects. Sometimes the patient experiences slight light sensitivity for several hours after the procedure, and dilating drops can increase eye pressure, leading to nausea with headache. Those who feel seriously unwell are advised to consult a doctor immediately.
Adults don't need special training to the test. However, children may need it in the form of atropinization (pupil dilation) depending on age, previous experience and level of trust in the doctor. The whole procedure takes about 5 minutes.
Research result
During the examination, the ophthalmologist visually assesses the quality and condition of the eye structures to detect possible problems. Some models of slit lamps have a photo and video module that record the examination process. If the doctor finds that the results are not normal, this may indicate the following diagnoses:
- inflammation;
- infection;
- increased pressure in the eye;
- pathological change in the ophthalmic arteries or veins.
For example, in macular degeneration, the doctor will find drusen (optic disc calcifications), which are yellow deposits that can form in the macula, an area on the retina, early in the disease. If the doctor suspects a certain vision problem, he will recommend further detailed examination to make a final diagnosis.
Biomicroscopy is a modern and highly informative method of examination in ophthalmology, allowing a detailed examination of the ocular structures of the anterior and posterior sections under different lighting and image magnification. As a rule, there is no need to prepare specially for this study. Thus, a five-minute procedure makes it possible to effectively monitor the health of the eye and prevent possible deviations in time.
(Greek, bios life + mikros small + skopeo observe, explore) - a special research method that makes it possible to examine in detail the optical refractive media and tissue of the eyeball.
B. g. was first proposed by A. Gullstrand in 1911. The method is based on the phenomenon of light contrast (Tyndall phenomenon).
With B.'s help, you can detect the smallest changes in the eye caused by disease or injury, and diagnose very small foreign bodies. The method is of great value in the diagnosis of a number of eye diseases (for example, trachoma, glaucoma, cataracts, neoplasms of the visual organ, etc.).
The research is carried out using special device- slit lamp (see). The domestic slit lamp ShL-56 combines a powerful illuminator (500 thousand lux) and a binocular stereoscopic microscope with a resolution from X5 to X60. The microscope is placed directly in front of the tissue being examined, the illuminator is on the side. The angle between them is called the biomicroscopy angle. It varies within +60°. The study is carried out in a dark room. The sharp contrast between dark and lamp-lit areas of the eye allows you to see details that are indistinguishable under normal lighting.
In the process of B. g. are used following methods lighting: direct focal, parafocal, oscillatory, transmitted light, sliding beam, specular field. Using special devices, inspection can be carried out in infrared and ultraviolet spectral rays, fluorescent, polarized light.
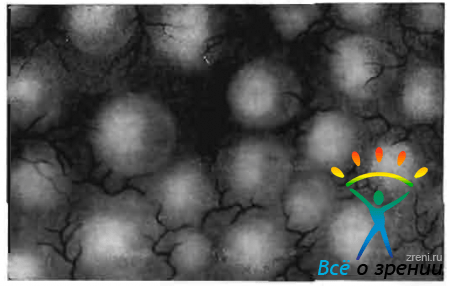
Rice. 1. Optical section of the cornea: a, b, c, d - anterior surface; d, f, g, h - rear surface; b - f and d - h - thickness of the cornea. Rice. 2. Turk's line during biomicroscopy (whitish dots): left -g in transmitted light; on the right - in an optical section of the cornea.
Examination in direct focal illumination allows obtaining an optical section (optical section) of the cornea, lens, vitreous body, retina and optic nerve head. The optical section of the cornea has the appearance of a slightly grayish, opalescent prism (Fig. 1), the width of the cut depends on the width of the beam of transmitted light. Normally, the incision is dotted with gray dots and streaks - this is what fibrils and nerves of the cornea look like when they are dissected by a beam of light. If there is an inflammatory focus or cloudiness in the cornea, an optical incision makes it possible to resolve the question of where exactly the pathological focus is located and how deeply the corneal tissue is affected. If available foreign body examination in an optical section helps to determine where it is located - in the cornea or penetrates into the eye cavity, which correctly guides the doctor in choosing the method of intervention.
With B. g., the Turk's line is easily detected, edges are found in 50% of cases during the study healthy eyes, mainly in children. The Turk's line is not constant; its formation and characteristic location are associated with the thermal flow of the intraocular fluid. Cooling of the fluid moving along the posterior surface of the cornea and, as a result, slowing down the speed of its flow leads to the deposition of cellular elements suspended in the chamber moisture on the cornea. The line is located on the posterior surface of the cornea, vertically below, and reaches the level of the lower pupillary edge. It consists of leukocytes and lymphocytes, the number of which ranges from 10 to 30. In transmitted light, the cellular elements look like translucent deposits; in direct focal light they take on the appearance of whitish dots (Fig. 2).

When focusing light and a microscope on the lens (direct focal light), an optical section of the lens is cut out in the form of a biconvex transparent body (see Lens). In the section, grayish oval stripes are visible - zones of separation caused by different densities of the lens substance (Fig. 3). The internal surfaces of the embryonic nucleus (1) with embryonic sutures, indicated in the figure by black Y-shaped lines, the outer surface of the embryonic nucleus (2), the surface of the senile nucleus (3), the cortex (4), the cleavage zones (5), the anterior and posterior surface of the lens (6). Studying the optical section of the lens makes it possible to see and accurately localize the delicate initial opacities of its substance, which has great importance in early diagnosis various kinds cataract.
Using the method of biomicroscopy of the vitreous body, fibrillar structures are identified in it gray(vitreous body), indistinguishable when examined by other methods. The study of these structures has a certain diagnostic value, especially for myopia.
Biomicroscopy of the fundus (bio-microophthalmoscopy), biomicroscopy of fundus tissues in the rays of the spectrum (biomicrochromoophthalmoscopy) open up new opportunities in ophthalmoscopic diagnostics (see Ophthalmoscopy). The use of direct focal light allows one to see an optical cross-section of the retina and optic nerve head. The retina is revealed in the form of a concave-convex translucent grayish strip located between the vitreous body and the choroid proper. The study of the optical section of the retina helps to diagnose and accurately localize small hemorrhages, vascular microaneurysms, and elements of tissue degeneration.
Optic disc during bio-microscopy due to the transparency of its forming nerve fibers visible to the cribriform plate of the sclera. Examination of the optic disc helps early differential diagnosis optic neuritis and stagnant nipple. Somewhat less opportunities open up with biomicroscopy of opaque parts of the eyeball, in particular the conjunctiva, iris, and choroid itself. However, in this case, B.'s method is an important addition to other methods of examining a patient with eye disease.
See also Examination of the patient (ophthalmological).
Bibliography: Koreyevich I. A. Biomicroscopy of the eye, Kyiv, 1969; Sh at l-pin N. B. Biomicroscopy of the eye, M., 1974; Berliner M. L. Biomicroscopy of the eye, v. 1-2, N.Y., 1949, bibliogr.; Kajiura M., Hashimoto H. a. T a k a h a s h i F. Recent advances in biomicroscopy of the fundus, Eye, Ear, Nose Tlir. Monthly, v. 53, p. 17, 1974.
N. B. Shulpina.
Biomicroscopy of the anterior segment of the eye is indicated for many pathologies. In fact, it is included in a standard ophthalmological examination, along with a check and examination of the fundus.
Injuries on the eyelids
Swelling or inflammation of the eyelids
Trauma to the eye area
Anomaly in the structure of the iris
Inflammation of the iris (and)
Dystrophic changes in the cornea and sclera
Hypertension (to assess the condition of the conjunctival vessels)
Endocrine diseases (especially diabetes mellitus)
Foreign bodies in any structure of the eye
Preparing for eye surgery
Postoperative examination
Evaluation of treatment results
Contraindications to biomicroscopy
Biomicroscopy of the eye is contraindicated in the following conditions:
Drug or alcohol intoxication
Mental illnesses accompanied by aggressive or inappropriate behavior
How is eye biomicroscopy performed?
Before the procedure, if it is necessary to examine deep structures (,), drops are instilled into the eyes. In case of examination of the cornea (its damage, inflammation or unknown pathology), a special dye is dripped into the eyes. After this, any eye drops are dripped, washing off the dye from unaffected areas (changes on the cornea remain stained a short time, allowing her to be examined). If it is necessary to remove a foreign body, then drops with an anesthetic are instilled before the examination (usually used).
The patient sits on a chair in front of the slit lamp, places the chin and forehead on special supports. The doctor takes a position opposite, on the other side of the lamp. The required illumination and the width of the light beam are set, after which the beam is directed into the eye being examined and the necessary structures are examined.
The procedure is absolutely painless. However, discomfort from the beam of light is also possible. Biomicroscopy of the eye takes about 10-15 minutes. During the procedure, it is recommended to blink as little as possible, which will speed up the examination process and increase its quality.
You can undergo an examination of the anterior segment of the eye in most public and private ophthalmology clinics.
26-07-2012, 20:39
Description
Research methodology
It does not present any difficulties, since the main parts of the conjunctiva are easily accessible to examination through a slit lamp. In some cases, when examining the conjunctiva of the eyelids, an assistant is needed whose role is to evert and hold the eyelids.
During biomicroscopy of the conjunctiva of the eyelids, it is often necessary to examine especially carefully transitional folds. When the upper eyelid is everted, the upper transitional fold does not protrude forward enough and, as a result, cannot be examined with due care. To facilitate the study of transitional folds, V.P. Filatov in 1923 proposed injecting 2 ml of a 0.5% novocaine solution under the conjunctiva. The transitional fold protrudes forward. Novocain straightens the folds of the conjunctiva, which makes the tissue more accessible to inspection. On the stretched conjunctiva, follicles, papillae and scars that develop with trachoma are better visible.
When biomicroscopy of the conjunctiva can be used almost all lighting options. A general view of the conjunctiva is usually performed under diffuse illumination under low microscope magnifications. Examination in an optical section with a narrow slit is advisable in the presence of edematous conjunctiva, follicular formations, and conjunctival cysts.
Silhouettes of the meibomian glands and cicatricial changes in the conjunctiva can be identified by examining the method of indirect illumination.
- Diaphanoscopic illumination helps in the differential diagnosis between translucent follicles and opaque papillary formations.
- The conjunctiva of the eyeball is a transparent, translucent tissue, so it can be examined in transmitted light. Rays of light penetrating freely through the conjunctiva fall on the underlying sclera. A strongly illuminated screen is formed, against which numerous conjunctival vessels and cystic formations are clearly visible.
- To study the state of the conjunctival vasculature, you can use a study in red-free light (green filter). In this case, the vessels appear more clearly in the form of dark branches on a blue or even green background.
- Examination with a sliding beam makes it possible to identify various types of irregularities on the surface of the conjunctival tissue.
- When using the mirror field method, the prominent formations of the conjunctiva give a clearly visible, peculiar intense brilliant reflex.
The conjunctiva is normal
Unchanged conjunctiva When examined with a slit lamp, the eyelid has a smooth, shiny surface without folds or thickenings and appears translucent, which allows one to see its adenoid layer. The rich vascularization of the conjunctiva is noteworthy. The vessels of the conjunctiva of the eyelids are distinguished by the correct vertical arrangement of the main large branches. In diffuse light, perforating branches of blood vessels are visible, arising from arterial arches located in the thickness of the upper and lower eyelids, and posterior conjunctival vessels. On the upper eyelid, three zones of these vessels can be distinguished (Fig. 14).
Rice. 14. Zones of the posterior conjunctival vessels of the upper eyelid. 1-first zone; 2-second zone; 3-third zone.
First zone is represented by 8-10 rather short vascular trunks arising from the marginal arterial arch of the upper eyelid and appearing on the conjunctiva 2 mm from the free edge of the eyelid. Second vascular zone consists of a smaller number of longer perforating branches originating from the peripheral arterial arch of the upper eyelid and appearing on the conjunctiva corresponding to the upper edge of the cartilage. Both vascular zones in the lower third of the conjunctiva of the upper eyelid anastomose with each other, forming in this place the third zone of connecting and intertwining vascular branches.
On the lower eyelid peripheral arterial arch is often absent, and upon examination of the conjunctiva, only one zone of the posterior conjunctival vessels is visible, originating from the marginal arterial arch of the eyelid. Many small branches arise from the main arterial trunks, forming a more superficial choroid plexus.
The conjunctiva of the sclera is transparent and is recognized mainly by the existing vessels. With biomicroscopy it is possible to distinguish two vascular systems(Fig. 15).

Rice. 15. Vessels of the conjunctiva of the eyeball (optical section).
One of them, more superficial, subepithelial, consists of posterior conjunctival vessels, passing from the conjunctiva of the eyelid and anastomosing in the circumference of the limbus with the anterior conjunctival vessels. These vessels lie in the superficial parts of the optical section of the conjunctiva. Another vascular system is located deeper and belongs to the episcleral category. These vascular systems differ not only in the depth of their location, but also in the color of the vascular trunks, their caliber, and the possibility of displacement along with the conjunctiva of the eyeball during blinking movements of the eyelids.
Superficial vessels of the conjunctiva They are bright red in color, quite thin and branched, and easily move along with the conjunctiva as it slides along the surface of the eyeball.
In most of these vessels it is usually visible granular blood flow- a physiological phenomenon. It is not always possible to distinguish an artery from a vein by the direction of blood flow, since it changes from time to time. In some cases, especially with vasodilation, oscillatory movements of the blood column in one direction or another and a complete stop of blood flow are observed - a phenomenon of stasis. When vasoconstrictors, in particular adrenaline, are instilled, the granular cryo-current is restored.
Deeper located vessels are more saturated in color and larger in caliber. When the conjunctiva is displaced, they do not change their location. Distinguish episcleral artery from vein often quite difficult, since the difference in their color is subtle, and the direction of blood flow is almost impossible to determine due to the significant width of the vessels.
In the limbus area the conjunctiva imperceptibly passes into the transparent tissue of the cornea. For many, during biomicroscopy, especially in the area of the upper and lower limbus, one can see this transition in the form of peculiar radial stripes of a whitish color: between these stripes - strands of the conjunctiva - transparent areas of tissue of the cornea are clearly visible. Alternating transparent and opaque zones will give the limb a characteristic striation. This is the so-called palisade zone (Fig. 16).

Rice. 16. Palisade area.
Sometimes pigment is deposited on this zone, making the radial striations appear more clearly.
In the area of the limbus, biomicroscopy reveals a very rich network of vessels with a unique architecture, which are mainly branches of the anterior conjunctival arteries and veins. Here you can also highlight three vascular zones(Fig. 17).

Rice. 17. Limbal vessels.
- The first, most peripherally located zone of the palisades is characterized by the presence of parallel, non-anastomosing vascular branches located about the corresponding radial recesses of the limbus. Its length is 1 mm.
- Further towards the cornea there is a second, middle zone, characterized by a large number of anastomosing vessels. Its length is 0.5 mm.
- The third - the zone of terminal capillaries - occupies a space equal to 0.2 mm.
Normally, no matter how wide the limbus is, the terminal capillaries do not penetrate into the transparent tissue of the cornea. One of them does not end freely. At the top of each vascular loop (terminal capillary), the direction of blood flow changes, becomes reversed, and the vessel itself expands. This is the beginning of the venous knee of the capillary.
Biomicroscopy of limbal vessels plays an important role in the early diagnosis of trachoma.
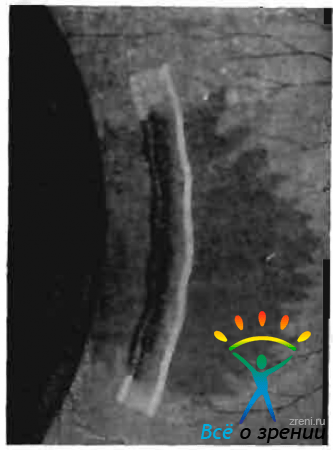
When examining the limbal and perilimbal area, you can see vessels containing very light (liquefied) blood, and sometimes colorless liquid. This water veins, described in 1912 by Ascher. Histologically it was found that they originate from the scleral wall of Schlemm’s canal, pierce the sclera in an oblique direction and appear on it outer surface in Limb Circumference.
Water veins visible in every third or fourth patient, mainly in the area of the palpebral fissure, slightly above or below the horizontal meridian of the eye. The number of visible veins varies individually. If it is not always possible to immediately notice a vein, then the conjunctival or episcleral vessel that perceives it is usually clearly visible. In some of these vessels it is possible to see two fractions of liquid, different in color (blood and transparent aqueous humor). In these cases the vessel appears two-layer, and sometimes three-layer (Fig. 18).

Rice. 18. Water vein.
When the endothelial septa disappear between these layers, the fluids stick together into one common current and the vessel (vein) takes on a light pink and then its normal red color. If you trace the course of such a vessel to the limbus, you can see the water vein.
During long-term observation of the place where the water vein flows into the receiving vessel, Z. A. Kaminskaya (1950) saw a phenomenon she called piston phenomenon. From time to time, often synchronously with the pulse, a small column of blood flows into the aqueous vein and then flows back. This phenomenon resembles a pump that seems to pump out the intraocular fluid contained in the aqueous vein. According to Z.L. Kaminskaya, the piston phenomenon plays a certain role in the mechanism of drainage of intraocular fluid along the anterior outflow tract.
When biomicroscopy of the conjunctiva, especially with glaucoma, attention should be paid anterior ciliary vessels associated with scleral emissaries. They are visible at some distance from the limb. Arteries enter the eye, veins exit from it.
It is difficult to distinguish an artery from a vein even with a slit lamp. The artery is usually more tortuous than the vein and has fewer lateral branches. To more accurately differentiate an artery from a vein, you need to thread the vessel (after instilling anesthetics) with the edge of a glass rod. If the central segment of the vessel expands and fills with blood, then it is a vein; if the peripheral segment, then the vessel is an artery.
With age the conjunctiva undergoes changes. In older people, there is a thinning of the optical section of the conjunctiva, a decrease in the transparency of the tissue, which acquires a yellowish tint. In the area of the palpebral fissure in the conjunctiva of the eyeball, fatty and hyaline deposits are often observed. The conjunctival and episcleral vessels become denser and become tortuous. When examined in an optical section, it is clear that they lift the conjunctival tissue above themselves, protruding above its surface. Often happens varicose veins vessels with the formation of petechiae.
Pathological changes in the conjunctiva
Diseases of the conjunctiva occupy one of the leading places among other types of eye pathology, accounting, according to various authors, from 30 to 47% of total number eye diseases.
Inflammatory diseases
The conjunctiva is in wide contact with the external environment and is therefore most susceptible inflammatory diseases associated with the introduction of exogenous infection.
Trachoma
Trachoma- chronic infectious proliferative inflammation of the conjunctiva, characterized by tissue hypertrophy with the development of follicles and papillae in it and ending with scarring.
Trachoma belongs to the group of diseases for which biomicroscopy is leading research method throughout clinical course process. Microscopy is necessary for the early diagnosis of trachoma, determining its stage, monitoring the dynamics of the disease under the influence of tone or other therapy, which makes it possible to determine when it is necessary to strengthen, weaken or change the treatment. Biomicroscopy plays a big role in determining whether a patient is cured. Dynamic observation of patients with trachoma shows that in most cases only biomicroscopic examination makes it possible to establish the true recovery of the patient, the complete elimination of the trachomatous process.
Clinical manifestations of trachoma varied - from pronounced to subtle changes in the area of the conjunctiva and limbus. There are erased and mild forms of trachoma. In the latter case, biomicroscopic examination is extremely important for epidemiological reasons.
When examining a patient with the naked eye in the early, initial stage of trachoma, the conjunctiva in some cases may appear almost unchanged. The researcher's attention is attracted only red dots on conjunctival cartilage.
- When biomicroscopy, these points appear as expanded, newly formed capillaries extending from the main vascular trunks of the conjunctiva and their branches in a direction perpendicular to the conjunctival surface. As the process develops, each of these vessels begins to branch, forming capillary arches (vascular bouquets), located parallel to the surface of the connective membrane.
- When examined in an optical section, it is clear that the vessels lie under the epithelium in the adenoid tissue of the conjunctiva. A conjunctival papilla is formed in the circumference of each vascular trunk. Group accumulations of hypertrophied papillae are more often visible on the conjunctiva of the cartilage of the upper eyelid, mainly in the area of the corners of the eyelids. where in connection with this a peculiar mosaic picture arises.
However, early biomicroscopic diagnosis of trachoma, based only on the observation of an increase in the number and hypertrophy of the papillary formations of the conjunctiva, may be erroneous. Papillary hypertrophy It is also observed in a number of commonplace chronic conjunctivitis with a benign course and a favorable outcome.
Dynamic observation of patients with trachoma soon after the detection of hypertrophy and an increase in the number of papillae, and sometimes in parallel with them, allows us to identify the presence follicles. They appear on the conjunctiva of the transitional fold, and then on the cartilage, located in the diffusely infiltrated tissue between the papillae, as if pushing them apart and pressing them to the sides (Fig. 19).

Rice. 19. Stage I trachoma. Changes in the conjunctiva of the eyelid.
Follicles, unlike papillae, develop not only in the conjunctiva of the eyelids, but also on the lacrimal caruncle and the semilunar fold.
Initial follicles have the appearance of gray, slightly protruding above the surface of the conjunctiva, vaguely contoured formations, located mainly in places of bifurcation of blood vessels; they do not yet have their own vessels. As each follicle grows and matures, newly formed vessels are directed to it from the surrounding tissue, which weave around it like a mesh, at the same time giving branches that penetrate into the depths of its tissue.
In some cases distinguishing papillae from follicles is not easy. An inexperienced researcher may mistake the papillae for follicles and vice versa. In order to correctly recognize them during examination with a slit lamp and correct interpretation of the process, it is recommended to dry the surface of the conjunctiva before the examination using a damp sterile swab, removing the existing mucus deposits and tears. When differentiating a papilla from a follicle, the appearance of the formation, its size, shape, color, degree of transparency, and nature of vascularization are taken into account.
The conjunctival papilla is smaller in size compared to the follicle, polygonal shape, a more saturated red color. Its fabric is only relatively transparent. The pattern of vascularization of the papilla is typical. The feeding vessel is located inside it (in the center or slightly eccentric, Fig. 20),

Rice. 20. Stage I trachoma. Papillae of the conjunctiva of the eyelid (optical section).
The appearance of the vessel usually precedes the formation of the papilla.
Trachomatous follicle 4-6 times larger than the papilla, has a spherical shape, gray-yellow color. Its tissue is more transparent than the tissue of the papilla. The follicle has a sharply different type of vascularization from the papilla. The vessels are located mainly on the surface of the follicle (Fig. 21)

Rice. 21. Stage I trachoma. Follicles of the conjunctiva of the eyelid (optical section).
and develop later than the follicle itself.
In the first stage of trachoma, in addition to follicles and papillae, biomicroscopic examination reveals changes in the epithelium and diffuse cellular infiltration of adenoid subepithelial tissue. The layers of the epithelium are thickened and less transparent than normal. Adenoid tissue is swollen, loose, granular, which makes the optical section of the conjunctiva much thicker and less transparent. In the vessels of the conjunctiva there is stagnation of blood with the presence of small hemorrhages in the circumference. The correct flow of blood vessels is disrupted, and numerous anastomoses appear between them.
In stage II of trachoma many papillae undergo reverse development. Only in the papillary form of trachoma is a well-developed mosaic of papillae visible throughout the cartilage conjunctiva. There is an increase in the number of follicles, but at the same time, some of them undergo liquefaction necrosis in the center. Such follicles acquire a dull gray color, unclear boundaries, and often open. The scarring process begins.
Helps identify initial, even hidden, deep scars maximum narrowing of the lighting gap and maximum brightness of the light beam during biomicroscopy. The scars that appear at the site of the follicles look like very delicate white lines located between the papillae. They must be distinguished from between the papillary fissures, which are usually filled with mucus and leukocytes.
In the circumference of the scars there is a significant number of newly formed vessels (Fig. 22).

Rice. 22. Scars of the conjunctiva of the eyelid with trachoma.
In stage III trachoma is characterized by progressive scarring, leading to connective tissue replacement of the affected conjunctiva. With biomicroscopy, islands of infiltration and hypertrophied papillae are visible among smooth, shiny, well-defined scars.
For trachoma stage IV cicatricial cords of a silvery appearance are found, located mainly in areas of richer vascularization of the conjunctiva. Severe scarring of the conjunctival tissue is noted in the area of the sulcus subtarsalis, i.e. there. where the main trunks of the posterior conjunctival vessels arise, as well as in the area of anastomoses between individual vascular branches. Scars are usually located along the vessels or cross them at an angle. In the latter case, the scars stand out more prominently against the background of the vascular trunks.
In the end untreated or poorly treated trachoma Scar tissue completely interferes with all follicles and papillae and leads to obliteration of blood vessels. In these cases, it is impossible to obtain an optical section of the conjunctiva in the area of the formed scar.
In the end successfully treated trachoma Scars also develop, but they are gentle, translucent, do not tighten the conjunctival tissue, and do not lead to the closure of the excretory ducts of the conjunctival glands. Against the background of such scars, the conjunctival section appears almost normal. Scars can only be seen by the delicate silvery layers of denser tissue visible on different depths optical cut.
Biomicroscopic studies have proven that with trachoma, in parallel with changes in the conjunctiva, and sometimes even preceding them, changes in limbo. Superficial, diffuse vascular keratitis, or pannus, occurs.
It allowed us to come to a correct understanding of the trachomatous process of the cornea and regard it not as a complication, but as one of the components of the sometimes early clinical manifestation of trachoma. It has been proven that in some cases the cornea may be the site of primary localization of the trachomatous virus.
According to the observation of a number of authors (L. S. Slutskin, 1940; N. N. Nurmamedov, 1960), damage to the cornea during the trachomatous process during the study slit lamp observed in 95-100% of patients. When examined using conventional methods with the naked eye, pannus is detected in only 7-10% of patients (V.V. Chirkovsky, 1953).
When examined using a slit lamp, it is clear that in the early stages of trachoma the transparency of the upper limb decreases, and its characteristic radial striation disappears. The limbus acquires a grayish tint and protrudes slightly above. surface of the cornea, its border becomes uneven. The vessels of the limbus are usually filled with blood and are visible down to the smallest branches.
Soon, when examining in transmitted light in the region of the upper limb, one can notice very mild cloud-like opacification of the cornea, consisting of a mass of gray dots and thin threads. In an optical section, the corneal tissue in this zone appears opalescent, opacities are located in the subepithelial zone. The number of limbal vessels increases, from which capillaries extend, penetrating into the corneal tissue along grayish infiltrating threads. These vessels, like the infiltrates, lie very superficially (Fig. 23).

Fig. 23. Trachomatous pannus (optical section)
Pannus vessels consist mainly of tortuous, densely branching veins; the artery has a more linear course and is located deeper.
Somewhat later, in the limbus zone, you can see small, round, grayish gelatinous islands - follicles. They, just like the follicles of the conjunctiva, go through the entire cycle of their development; in some cases they have abortive development. Follicles often merged together form a zone of pronounced infiltration, visible to the naked eye. As a result, small scar impressions covered with epithelium remain in place of the follicles. These impressions are facets, also known as “eyes”, arise as a result of degeneration and disintegration of trachomatous follicles.
With a malignant course of pannus, its ulceration, infiltration and vessels penetrate into the deeper layers of the cornea. In such cases, they are visible in the middle and deep parts of the optical section. In this case, changes of a secondary nature may also develop - deposition of calcium and lipoids in the affected cornea. As a result of trachomatous pannus, a more or less intense clouding of the cornea with a tendon tint remains. Permeated with vessels.
When diagnosing trachoma, one must take into account the possibility of mixing this disease with others. inflammatory lesions conjunctiva.
When differential diagnosis of trachoma with follicular conjunctivitis, it should be taken into account that when follicular conjunctivitis there is no diffuse infiltration of subepithelial tissue and hypertrophied papillae. When examined with a slit lamp, the follicles appear small, transparent, and do not have a developed network of capillaries (Fig. 24).
Rice. 24. Follicular conjunctivitis.
With follicular conjunctivitis, the same as with acute conjunctivitis of another origin, thickening of the limbus, expansion of the terminal capillaries and a slight lengthening of individual capillary loops may be observed. However, these changes soon disappear. Biomicroscopic examination does not detect either newly formed vessels or infiltration in the corneal tissue. There is no pannus with follicular conjunctivitis; There is no scarring of the conjunctiva as a result of the disease. After the process is eliminated, the conjunctival tissue appears completely unchanged.
In the differential diagnosis of trachoma with spring catarrh the pale, sometimes milky-white color of the conjunctiva, characteristic of the latter, and the predominant localization of changes on the conjunctiva of the cartilage of the upper eyelid (tarsal form) are taken into account. A lethal examination of these changes by bioncroscopy can be carried out only after removing a thick coating of viscous secretion from their surface.
Macroscopically revealed uneven surface of the conjunctiva. This is explained by the presence of dense, pale, shiny, as if polished, formations. These growths are known to be based on hyaline degeneration of subepithelial tissue.
Hyaline growths on the conjunctiva during spring catarrh they are fused, degeneratively degenerated papillae. When examined with a slit lamp, they look like multiple flat, polygonal and oval formations adjacent to each other with a smooth surface. Vascular bundles are visible, extending from large arterial trunks and running perpendicular to the surface of the conjunctiva. From these bundles a more superficial network of vessels arises (Fig. 25, a).

Rice. 25. Spring catarrh. a - tarsal form: b - limbal form.
Unlike papillae in spring catarrh papillae in trachoma smaller in size, red in color, more cloudy and lacking shine due to infiltration and desquamation of the epithelium. In addition, the papillae in trachoma never merge into one continuous mass. Each is formed around one vascular trunk and is separated from neighboring formations by a more or less narrow gap.
In some cases it is necessary to differentiate trachomatous pannus with limbal form of vernal catarrh. With joyful catarrh, changes occur around the entire limbus, and not just in its upper half, as with trachoma. At the limbus, small grayish islands are formed, consisting of a hyaline glassy substance, which is faintly translucent when examined in direct focal light. Often they merge and form a continuous ridge with a bumpy surface, sometimes moving onto the cornea (Fig. 25, b). Vascularization of vitreous formations is very insignificant compared to vascularization in trachomatous pannus. The limbal vessels usually pass through them at varying depths and terminate singly on the cornea.
With spring catarrh Damage to more centrally located parts of the cornea is also observed. Here, in the most superficial layers, very small, flat, scaly deposits of gray-white color appear. When the eyelids blink, these scales can be washed away with tears and erosions remain in their place. It is believed that these are neurotically degenerated elements of the epithelium of the cornea. Their favorite location is the upper half of the cornea (under the upper eyelid) and the palpebral fissure area.
It should not be forgotten that with the limbal form of spring catarrh conjunctival cartilage is often involved in the process. It acquires a milky white hue, against which even under low microscope magnification a typical mosaic of papillae is observed. They also show hyaline degeneration of the tissue, which gives the papillae a peculiar, glassy, translucent appearance.
At the end of spring catarrh all symptoms disappear without a trace; unlike trachoma, there is no scarring. Changes in the limbus and cornea also undergo complete reversal. As a result, retrospective diagnosis of vernal catarrh with a slit lamp is very difficult.
Dystrophic changes
Pinguecula- hyaline degeneration of the conjunctiva. It has the appearance of a yellow island, most often located at the inner limb of the cornea. Biomicroscopic examination in direct focal light reveals that the process of degeneration involves the deep sections of the optical section of the conjunctiva. Vitreous amorphous masses are also revealed under the cut of the conjunctiva. Sometimes small cavities are visible in the pinguecula tissue (Fig. 26).

Rice. 26. Pinguecula.
Pterygium, or pterygoid hymen, is a fairly common dystrophic change in the conjunctiva. When examining with a slit lamp Special attention You should pay attention to examining the head of the pterygium, i.e., that part of it that is located on the cornea.
There are two zones in the head of the pterygium: vascular and avascular (Fig. 27).
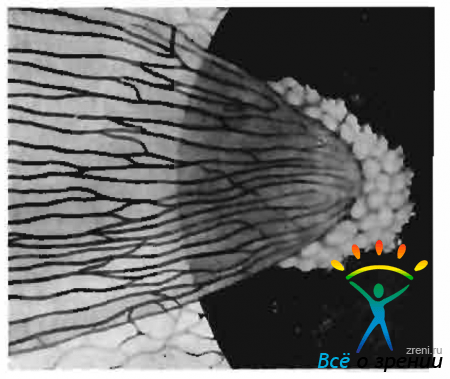
Rice. 27. Pterygium.
The latter is located in front of the vascular zone (towards the center of the cornea) and consists of foci of gelatinous cloudiness, the processes of which extend into the deeper parts of the corneal stroma.
Biomicroscopic examination allows you to determine whether the pterygium is stationary or progressive, which helps to correctly decide on the timing and type of surgical intervention. Stationary pterygium is characterized by a mildly defined, flat, avascular zone of the head, which imperceptibly merges with the tissue of the cornea. With progressive pterygium, the avascular zone is more pronounced, loosened and noticeably rises above the surface of the cornea. In front of the head of the pterygium there are sometimes punctate subepithelial opacities.
Differential diagnosis of pterygium with the initial form of Bowen's epithelioma - see below.
Neoplasms
Papilloma- a benign fibroepithelial formation, most often localized on the conjunctiva of the eyelids around the lacrimal caruncle, less often on the conjunctiva of the eyeball. The tumor is pink in color, soft in consistency, loosely fused to the underlying tissues, and often pedunculated.
Biomicroscopy reveals that the surface of the neoplasm is uneven and represents a conglomerate of papillomatous growths of a mosaic nature. With your look the tumor resembles a mulberry or cauliflower(Fig. 28).

Rice. 28. Papilloma of the conjunctiva.
Papilloma tissue does not transmit light from a slit lamp, which makes it impossible to obtain an optical section during bioncroscopy. Papilloma is characterized by rather sparse vascularization; it lacks glomerular vascular formations typical of malignant and vascular tumors.
When papilloma is localized at the limbus, it is necessary to carry out differential diagnosis with carcinoma.
Epithelioma, or carcinoma, - malignant epithelial tumor of the conjunctiva; prone to active growth and relapse after removal. The tumor is localized, as a rule, in the circumference of the limbus. In the initial stage, it is difficult to distinguish it from papilloma, pinguecula and incipient pterygium.
During biomicroscopic examination The hallmark of epithelioma is tuberosity, lobulation of the tumor. Ulceration of the surface is often observed, which is determined by the presence of a defect in the optical section of the conjunctiva. This sign is especially well revealed after staining the surface of the epithelioma with a fluorescein solution. In the differential diagnosis of epithelioma, great importance should be attached to slit-lamp examination nature of vascularization.
Epithelioma is richly vascularized. Each tumor lobule is equipped with a central vessel with a mass of capillary branches. The vessel penetrating the tumor lobule rises to its apex and then descends back (Fig. 29).

Rice. 29. Epithelioma of the conjunctiva.
Basal capillaries form a common vascular network, which, with its numerous anastomoses, feeds all tumor lobules. This type of vascularization is pathognomonic for epithelioma.
Epithelioma of intraepithelial localization, without disturbing the basement membrane of the epithelial layer, stands out as a separate form of precancerous dyskeratosis - Boveia epithelioma. The formation has the appearance of a grayish-white flat plaque, localized, as a rule, in the circumferential limbus. When examined using a slit lamp, an uneven surface of the neoplasm is noted, which is revealed by a break in the light slit, a significant number of white scales of exfoliating epithelium (dyskeratosis). The boundaries of the tumor are clear. With epithelioma of Boveia there is a pronounced vascular reaction from the surrounding conjunctiva
Nevus, or birthmark , conjunctiva does not belong to the category of true tumors. Characterized by slow growth during the development of the organism, in adults it becomes stationary. However, in some cases, malignant degeneration of the nevus tissue is possible as a result of irritation, trauma to the nevus, and sometimes for no apparent reason.
Nevus is most often localized on the conjunctiva of the sclera in the limbus. It can appear in a pigmented or non-pigmented form, which causes different colors of the spots - from dark brown to light yellow.
Biomicroscopy in direct focal light and with a grazing beam reveals flat or very slightly protruding lesion on the surface of the sclera, with fairly clear boundaries (Fig. 30).
Rice. thirty. Nevus of the conjunctiva.
The tissue is characterized by delicate dusty pigmentation. With a narrow gap, you can determine the depth of the pigment and find out whether the nevus is epithelial or subepithelial. With subepithelial localization, pigment islands are visible in an optical section under the epithelial strip. Sometimes there is a nevus with vacuolar degeneration - the so-called naeviis cysticus. In an optical section with this form of nevus, numerous transparent cavities are visible - vacuoles, separated by thin partitions.
The nonvesicular tissue contains vessels, but they are few in number and do not provide dense branching.
A thorough biomicroscopy makes possible to carry out differential diagnosis between nevus and incipient melanoblastoma of the conjunctiva. A big role in this belongs to the observation of changes in the nature of vascularization. The discovery of new vascular branches in the non-vesical tissue is suspicious regarding its malignant degeneration. Simultaneously with the change in the nature of vascularization or somewhat later, an increase in the size of the neoplasm, increased pigmentation of the tissue, and redistribution of pigment are noted.
Melanoblastoma of the conjunctiva belongs to the most malignant tumors, has a tendency to metastasize. She. arises spontaneously or develops from a conjunctival nevus. The tumor is most often localized near the limbus, but is also observed in the area of the lacrimal caruncle, the semilunar fold of the conjunctiva. Melanoblastoma spreads quite quickly, giving rise to daughter growth nodes.
Biomicroscopy reveals the lobular structure of the tumor tissue and its increased pigmentation. Unlike a nevus, the pigment of melanoblastoma is coarser and lumpy. When attempting to obtain an optical section in the area of melanoblastoma, the density of the tumor tissue and its intimate adhesion to the underlying scleron are noted. The light beam usually penetrates poorly into the tumor mass. A characteristic biomicroscopic sign of melanoblastoma is its lush vascularization, which is not observed with nevus. A branching bundle of capillary vessels is visible in the center of each tumor lobule. In addition, a rich vascular network is observed deep in the tumor.
Here is one of our clinical observations, where slit lamp examination significantly helped to make the correct diagnosis.
Patient S., 30 years old. was admitted to the hospital for neoplasms of the conjunctiva of the right eye. Marked on the eyeball since childhood age spot, V last years it began to increase in size and stand above the surface of the eye.
Upon examination, uneven distribution was found in the upper parts of the limbus pigmented formation of the conjunctiva with an elastic consistency, round shape measuring 4X6 mm. The remaining parts of the eyeball are unchanged. Visual acuity 1.0.
When examined with a slit lamp in direct focal illumination, it is clearly visible that the neoplasm has a lumpy surface. It is not possible to obtain an optical section of the tissue, which emphasizes its density. There is pronounced vascularization of the neoplasm (a large number of newly formed vascular loops). There is a lot of coarse lumpy pigment in the tumor tissue (Fig. 31, a).

Rice. 31. Melanoblastoma of the conjunctiva. a - biomicroscopic picture; b - histological picture (hematoxylin-tosin staining, magnification 10 X 20).
Diagnosis: conjunctival melanoblastoma developing from a nevus. Biomicroscopy under fluorescent lighting and a study with radioactive phosphorus, which showed a high level of P accumulation, confirmed the diagnosis.
Produced melanoblastoma removal with preliminary and sequential diathermocoagulation of surrounding tissues. Histological examination revealed melanoblastoma of the alveolar structure with lush growth in central departments. Cellular and nuclear atypia of the tumor tissue (epithelioid type of structure) was noted (Fig. 31. b).
Changes in glaucoma
Biomicroscopy of the conjunctiva of the eyeball is mandatory during a comprehensive examination of a patient with suspected glaucoma, as well as during dynamic monitoring of a patient with glaucoma. In both cases, it is necessary to pay attention to the condition of the anterior ciliary vessels (playing important role in the outflow of intraocular fluid), especially those located in the upper and lower parts eyeball. Changes in the vessels located within the palpebral fissure, often exposed to adverse environmental influences, can disorient the observer. These vessels, especially in older people, are often tortuous, their branches varicose.
In glaucoma, changes in both the anterior ciliary arteries and anterior ciliary veins are observed; the latter are changed more often in congestive glaucoma. Particular attention should be paid during biomicroscopy area of scleral openings- emissaries through which the anterior ciliary arteries enter the eye and the veins exit. In patients with glaucoma, it is sometimes necessary to observe peculiar changes called the emissary symptom.
Exists incomplete and complete emissary symptom, the first is more common than the second. An incomplete emissary symptom is expressed in an increase in the size of the scleral opening by 2-3 times. When bnomncroscopy, it looks like a grayish round spot, in the center of which (in some cases eccentrically) is the anterior ciliary vessel. Sometimes, next to the expanded emissary, there are delicate accumulations of pigment brought here by the flowing chamber moisture.
With a complete emissary symptom above the enlarged scleral opening there is elevation, swelling of the conjunctiva (Fig. 32),

Rice. 32. Complete symptom emissary for glaucoma.
similar to that observed after fistulizing antiglaucomatous operations. In some cases, such a conjunctival “pad” does not appear above the emissary itself, but slightly away from it. Its development is associated with the detachment of the conjunctiva from the sclera by intraocular fluid flowing through the emissary. Direct focal light examination reveals a layer of clear fluid under the conjunctiva. When the anterior ciliary vessel is located near the limbus, the appearance of the emissary symptom is usually not accompanied by the formation of a typical conjunctival pad, since the latter in the limbus area is quite tightly fused to the underlying sclera. Under these conditions, as a rule, only a barely noticeable raised conjunctival ridge appears.
Detection of the Emissary Symptom during biomicroscopy obliges the doctor to suspect the presence of a glaucomatous process. If during examination of the patient the intraocular pressure turns out to be normal, then special tests should be performed to detect glaucoma. Under load conditions, compensation due to expansion of the emissary is often insufficient, which is reflected in an increase in intraocular pressure.
In relatively young patients, when the sclera is not yet so dense, the emissary symptom occurs more often in the early stages of glaucoma or in a preglaucomatous state. In elderly patients, due to thickening of the outer membrane of the eye, the emissary symptom appears in the later stages of glaucoma against the background dystrophic changes sclera. The sclera around the anterior ciliary vessel is sometimes reduced and thinned to such an extent that the choroid becomes visible through the opening.
In the diagnosis of glaucoma, it may be of certain importance monitoring the condition of the water veins. TO early signs Glaucoma, according to Z. A. Kaminskaya, refers to the appearance of a negative phenomenon of low tide. When a vessel receiving an aqueous vein is compressed with a glass rod, a twofold reaction can be observed: either the vein remains transparent and the intraocular fluid fills the vessel receiving the vein (positive ebb phenomenon), or the vein fills with blood (negative ebb phenomenon).
In addition to the negative phenomenon of low tide, glaucoma is characterized by "plus-minus" phenomenon. It consists in the fact that after squeezing the vessel receiving the water vein, the vein initially remains transparent and then fills with blood. With glaucoma in a state of decompensation, all aqueous veins are filled with blood, and the piston phenomenon is absent.
It must be performed on patients who have undergone fistulizing antiglaucomatous surgery. After trephination of the sclera according to Elliott, anterior sclerectomy, and iridenkleisis surgery, a filtration pad, sometimes a multi-chamber one, is formed over the upper limbus. When examined in direct focal light, it is clear that its cavities are filled with transparent intraocular fluid. Through them you can see the filtering surgical opening in the sclera and clumps of pigment.
- With a well-expressed filtering postoperative scar Normal intraocular pressure values are usually observed.
- With unsatisfactory filtration, the surgical scar appears flat, abundantly vascularized due to newly formed conjunctival and episcleral vessels.
Article from the book: .