Acute heart failure: what is it, symptoms, treatment, causes, signs, help. Heart failure
RCHD (Republican Center for Health Development of the Ministry of Health of the Republic of Kazakhstan)
Version: Clinical Protocols of the Ministry of Health of the Republic of Kazakhstan - 2013
Acute transmural myocardial infarction of other specified sites (I21.2)
Cardiology
general information
Short description
Approved by the minutes of the meeting
Expert Commission on Health Development of the Ministry of Health of the Republic of Kazakhstan
No. 13 dated 06/28/2013
Acute heart failure (AHF)- AHF - a clinical syndrome characterized by the rapid onset of symptoms that determine a violation of the systolic and / or diastolic function of the heart (decreased CO, insufficient tissue perfusion, increased pressure in the capillaries of the lungs, stagnation in the tissues).
Allocate for the first time AHF (de novo) in patients without a known history of cardiac dysfunction, as well as acute decompensation of CHF. At rapid development AHF, in contrast to the gradually increasing symptoms and acute decompensation of CHF, there are usually no signs of fluid retention in the body (Recommendations of the European Society of Cardiology for the diagnosis and treatment of acute and chronic heart failure, 2012).
I. INTRODUCTION
Protocol name: Protocol for the diagnosis and treatment of acute heart failure
Protocol code:
ICD-10 codes:
I50 - Heart failure
I50.0 - Congestive heart failure
I50.1 - Left ventricular failure
I50.9 Heart failure, unspecified
R57.0 Cardiogenic shock
I21.0 - Acute transmural infarction of the anterior myocardial wall
I21.00 - Acute transmural infarction of the anterior wall of the myocardium with hypertension
I21.1 - Acute transmural infarction of inferior myocardial wall
I21.10 - Acute transmural infarction of inferior myocardial wall with hypertension
I21.2 - Acute transmural myocardial infarction of other specified sites
I21.20 - Acute transmural myocardial infarction of other specified sites with hypertension
I21.3 - Acute transmural myocardial infarction, unspecified
I21.30 - Acute transmural myocardial infarction, unspecified, with hypertension
I21.4 - Acute subendocardial myocardial infarction
I21.40 - Acute subendocardial myocardial infarction with hypertension
I21.9 - Acute myocardial infarction, unspecified
I21.90 - Acute myocardial infarction, unspecified with hypertension
I22.0 - Repeated infarction of the anterior myocardial wall
I22.00 Recurrent anterior myocardial infarction with hypertension
I22.1 - Recurrent infarction of inferior myocardial wall
I22.10 - Recurrent inferior myocardial infarction with hypertension
I22.8 - Recurrent myocardial infarction of other specified location
I22.80 - Recurrent myocardial infarction of another specified location with hypertension
I22.9 - Recurrent myocardial infarction, unspecified
I22.90 - Recurrent myocardial infarction of unspecified location with hypertension
I23.0 Hemopericardium as an immediate complication of acute myocardial infarction
I23.00 Hemopericardium as an immediate complication of acute myocardial infarction with hypertension
I23.1 Atrial septal defect as a current complication of acute myocardial infarction
I23.10 - Atrial septal defect as a current complication of acute myocardial infarction with hypertension
I23.2 Ventricular septal defect as a current complication of acute myocardial infarction
I23.20 Ventricular septal defect as a current complication of acute myocardial infarction with hypertension
I23.3 Rupture of the cardiac wall without hemopericardium as a current complication of acute myocardial infarction
I23.30 Rupture of the cardiac wall without hemopericardium as a current complication of acute myocardial infarction with hypertension
I23.4 Rupture of chorda tendon as current complication of acute myocardial infarction
I23.40 Rupture of chorda tendon as a current complication of acute myocardial infarction with hypertension
I23.5 Rupture of papillary muscle as current complication of acute myocardial infarction
I23.50 Rupture of the papillary muscle as a current complication of acute myocardial infarction with hypertension
I23.6 Thrombosis of the atrium, atrial appendage and ventricle as a current complication of acute myocardial infarction
I23.60 Atrial thrombosis of the atrial appendage and ventricle as a current complication of acute myocardial infarction with hypertension
I23.8 - Other ongoing complications of acute myocardial infarction
I23.80 - Other ongoing complications of acute myocardial infarction with hypertension
I24.1 - Dressler's syndrome
I24.10 - Dressler's syndrome with hypertension
I24.8 - Other forms of acute ischemic heart disease
I24.80 - Other forms of acute ischemic heart disease with hypertension
I24.9 Acute ischemic heart disease, unspecified
I24.90 Acute ischemic heart disease, unspecified
Abbreviations used in the protocol:
BP - blood pressure
APTT - activated partial thromboplastin time
BAB - beta-blockers
VACP - intra-aortic counterpulsator
DZLA - jamming pressure pulmonary artery
ACE inhibitor - angiotensin-converting enzyme inhibitor
IHD - ischemic heart disease
MI - myocardial infarction
LV - left ventricle
LA - pulmonary artery
HF - heart failure
CO - cardiac output
SBP - systolic blood pressure
SI - heart index
SPPP - spontaneous breathing with constant positive pressure
NVPV - non-invasive positive pressure ventilation
IVS - interventricular septum
IOC - minute volume of blood circulation
CAG - caranarangiography
TPVR - total peripheral vascular resistance
RV - right ventricle
TS- heart transplant
TLT - thrombolytic therapy
PE - pulmonary embolism
CHF - chronic heart failure
HR - heart rate
CVP - central venous pressure
ECG - electrocardiography
EKS - pacemaker
ECMO - extracorporeal membrane oxygenation
EchoCG - echocardiography
NYHA - New York Heart Association
CPAP - continuous positive airway pressure
NIPPV - non-invasive positive pressure ventilation
Protocol development date: April 2013
Protocol Users: cardiologists, cardiac surgeons, anesthesiologists-resuscitators, therapists
Indication of no conflict of interest: missing.
Table 1. Provoking factors and causes of acute heart failure 
Classification
Acute circulatory failure can be manifested by one of the following conditions:
I. Acute decompensated heart failure(de novo or as decompensation of CHF) with characteristic complaints and symptoms of AHF that is moderate and does not meet the criteria for cardiogenic shock, pulmonary edema, or hypertensive crisis.
II. Hypertensive heart failure: complaints and symptoms of heart failure accompany high blood pressure with relatively preserved LV function. There are no signs of pulmonary edema on chest X-ray.
III. Pulmonary edema(confirmed by chest x-ray) is accompanied by severe respiratory failure, orthopnea, wheezing in the lungs, while the level of blood oxygen saturation before treatment is usually less than 90%.
IV. Cardiogenic shock- an extreme manifestation of AHF. This is a clinical syndrome in which, along with a decrease in systolic blood pressure less than 90-100 mm Hg. there are signs of reduced perfusion of organs and tissues (cold skin, oligoanuria, lethargy and lethargy). At the same time, the cardiac index is reduced (usually 2.2 l / min per 1 m2) and the pulmonary artery wedge pressure is increased (> 18-20 mm Hg). The latter distinguishes cardiogenic shock from a similar condition that occurs with hypovolemia. The main link in the pathogenesis of cardiogenic shock is a decrease in cardiac output, which cannot be compensated by peripheral vasoconstriction, which leads to a significant decrease in blood pressure and hypoperfusion. Accordingly, the main goals of treatment are to optimize the filling pressure of the ventricles of the heart, normalize blood pressure and eliminate the causes underlying the decrease in cardiac output.
V. HF with high cardiac output is characterized by elevated cardiac output with usually elevated heart rate (due to arrhythmias, thyrotoxicosis, anemia, Paget's disease, iatrogenic and other mechanisms), warm extremities, congestion in the lungs, and sometimes reduced blood pressure (as in septic shock).
VI. Right ventricular heart failure characterized by a syndrome of low cardiac output due to pumping failure of the pancreas (myocardial damage or high load - PE, etc.) with increased venous pressure in the jugular veins, hepatomegaly and arterial hypotension.
T. Killip classification(1967) is based on clinical signs and chest x-ray findings.
The classification applies primarily to heart failure in myocardial infarction, but may apply to de novo heart failure.
There are four stages (classes) of severity:
stage I- no signs of heart failure;
stage II- CH (wet rales in the lower half of the lung fields, tone III, signs of venous hypertension in the lungs);
stage III- severe HF (obvious pulmonary edema, moist rales spread to more than the lower half of the lung fields);
stage IV- cardiogenic shock (SBP 90 mm Hg with signs of peripheral vasoconstriction: oliguria, cyanosis, sweating).
J. S. Forrester classification(1977) is based on taking into account clinical signs that characterize the severity of peripheral hypoperfusion, the presence of congestion in the lungs, reduced cardiac index(SI) ≤ 2.2 L/min/m2 and elevated pulmonary artery wedge pressure (PWP) > 18 mmHg. Art.
Allocate the norm (group I), pulmonary edema (group II), hypovolemic and cardiogenic shock (group III and IV, respectively).
After stabilization of the condition, patients are assigned a functional class of heart failure according to NYHA
Table 2. NewYork Heart Association (NYHA) classification. 
Diagnostics
II. METHODS, APPROACHES AND PROCEDURES FOR DIAGNOSIS AND TREATMENT
List of basic and additional diagnostic measures
Table 1- List of basic and additional diagnostic measures 

Diagnostic criteria
Complaints and anamnesis:
Complaints are possible for shortness of breath / suffocation, dry cough, hemoptysis, fear of death. With the development of pulmonary edema, a cough appears with frothy sputum, often colored in pink color. The patient assumes a forced sitting position.
Physical examination:
During a physical examination, special attention should be paid to palpation and auscultation of the heart with the determination of the quality of heart sounds, the presence of III and IV tones, murmurs and their nature.
It is important to systematically assess the state of peripheral circulation, temperature skin, the degree of filling of the ventricles of the heart. RV filling pressure can be estimated using venous pressure measured in the superior vena cava. However, caution should be exercised when interpreting the result, since increased central venous pressure (CVP) may be due to impaired compliance of the veins and the pancreas with inadequate filling of the latter. Elevated LV filling pressure is usually indicated by the presence of crackles on lung auscultation and/or evidence of pulmonary congestion on chest x-ray. However, in a rapidly changing environment clinical evaluation the degree of filling of the left parts of the heart may be erroneous.
table 2- Clinical and hemodynamic signs in different types of AHF 
Note:* The difference between low CO syndrome and cardiogenic shock is subjective; when evaluating a particular patient, these classification points may partially coincide.
ECG
A 12-lead ECG can help determine the rhythm of the heart and sometimes help clarify the etiology of AHF.
Table 6 The most common ECG changes in HF. 

Chest x-ray
Chest x-ray should be performed as early as possible in all patients with AHF to assess the size and clarity of the heart shadow, as well as the severity of blood congestion in the lungs. This diagnostic study It is used both to confirm the diagnosis and to evaluate the effectiveness of treatment. Chest X-ray can distinguish left ventricular failure from inflammatory lung disease. It is important to take into account that radiological signs congestion in the lungs is not an accurate reflection of increased pressure in the pulmonary capillaries. They may be absent in PAWP up to 25 mm Hg. Art. and respond late to favorable hemodynamic changes associated with treatment (possible delay up to 12 hours).
Echocardiography (EchoCG)
EchoCG is necessary to determine the structural and functional changes underlying the DOS. It is used to assess and monitor the local and general function of the ventricles of the heart, the structure and function of the valves, the pathology of the pericardium, mechanical complications of MI, volumetric formations hearts. CO can be estimated from the speed of movement of the aortic or LA contours. With Doppler study - to determine the pressure in the LA (according to the jet of tricuspid regurgitation) and monitor the preload of the left ventricle. However, the validity of these measurements in AHF has not been verified by right heart catheterization (Table 4).
Table 4- Typical abnormalities detected by echocardiography in patients with heart failure 
The most important hemodynamic parameter is the LV EF, which reflects the contractility of the LV myocardium. As an "average" indicator, we can recommend a "normal" level of LV EF of 45%, calculated by the 2-dimensional EchoCG method according to Simpson.
Transesophageal echocardiography
Transesophageal echocardiography should not be considered as a routine diagnostic tool; it is usually resorted to only in case of obtaining an insufficiently clear image with transthoracic access, complicated valvular damage, suspected prosthesis malfunction mitral valve, to exclude thrombosis of the left atrial appendage at a high risk of thromboembolism.
Daily monitoring ECG (Holter monitoring)
Standard Holter ECG monitoring has a diagnostic meaning only in the presence of symptoms, probably associated with the presence of arrhythmias (subjective sensations of interruptions, accompanied by dizziness, fainting, a history of syncope, etc.).
Magnetic resonance imaging
Magnetic resonance imaging (MRI) is the most accurate method with maximum reproducibility of calculations for calculating the volume of the heart, its wall thickness and LV mass, surpassing echocardiography and radioisotope angiography (RIA) in this parameter. In addition, the method allows to detect thickening of the pericardium, to assess the extent of myocardial necrosis, the state of its blood supply and features of functioning. Conducting diagnostic MRI is justified only in cases of insufficient information content of other imaging techniques.
Radioisotope methods
Radionuclide ventriculography is considered to be very exact method determination of LV EF and is most often performed when studying myocardial perfusion to assess its viability and the degree of ischemia.
Indications for expert advice:
1. Consultation with an arrhythmologist - the presence of cardiac arrhythmias (paroxysmal atrial tachycardia, atrial fibrillation and flutter, sick sinus syndrome), diagnosed clinically, according to ECG and HMECG.
2. Consultation of a neurologist - the presence of episodes of convulsions, the presence of paresis, hemiparesis and other neurological disorders.
3. Consultation of an infectious disease specialist - the presence of signs infectious disease(pronounced catarrhal phenomena, diarrhea, vomiting, rash, change biochemical parameters blood, positive results of ELISA tests for intrauterine infections, markers of hepatitis).
4. Consultation with an ENT doctor - nosebleeds, signs of an upper respiratory tract infection, tonsillitis, sinusitis.
5. Consultation of a hematologist - the presence of anemia, thrombocytosis, thrombocytopenia, clotting disorders, other abnormalities of hemostasis.
6. Consultation of a nephrologist - the presence of data for UTI, signs of renal failure, decreased diuresis, proteinuria.
7. Consultation with a pulmonologist - the presence of concomitant lung pathology, decreased lung function.
8. Consultation with an ophthalmologist - scheduled inspection eye fundus.
Laboratory diagnostics
In all cases of severe AHF, invasive gas composition estimation arterial blood
with the determination of the parameters characterizing it (PO2, PCO2, pH, base deficiency).
In patients without very low CO and shock with vasoconstriction, pulse oximetry and end-tidal CO2 may be an alternative. The balance of oxygen supply and the need for it can be assessed by SvO2.
With cardiogenic shock and long-term existing syndrome small ejection, it is recommended to determine the PO2 of mixed venous blood in the LA.
Levels BNP and NT-proBNP in plasma increase due to their release from the ventricles of the heart in response to increased ventricular wall tension and volume overload. BNP > 100 pg/mL and NT-proBNP > 300 pg/mL have been suggested to be used to confirm and/or rule out CHF in patients admitted to the emergency department with dyspnea.
However, in elderly patients, these indicators have not been studied enough, and with the rapid development of AHF, their blood levels upon admission to the hospital may remain normal. In other cases, the normal content of BNP or NT-proBNP makes it possible to exclude the presence of CH with high accuracy.
If the concentration of BNP or NT-proBNP is increased, it is necessary to ensure the absence of other diseases, including renal failure and septicemia. A high level of BNP or NT-proBNP indicates a poor prognosis.
cardiac troponins are important in determining the diagnosis and risk stratification, as well as to enable the distinction between MI BP ST and unstable angina. Troponins are more specific and sensitive than traditional cardiospecific enzymes such as creatine kinase (CK), myocardial isoenzyme MB (MB-CK), and myoglobin.
An increase in the level of cardiac troponins reflects damage to myocardial cells, which in ACS BP ST may be the result of distal embolization of platelet thrombi from the site of rupture or tear of the plaque. Accordingly, troponin can be considered as a surrogate marker of active thrombus formation. If there are signs of myocardial ischemia (chest pain, ECG changes, or new wall motion abnormalities), an increase in troponin levels indicates MI. In patients with MI, the initial rise in troponins occurs within ~4 hours of onset of symptoms. Enhanced level troponins can persist for up to 2 weeks due to proteolysis of the contractile apparatus. There are no significant differences between troponin T and troponin I.
In blood healthy people even after excessive exercise, the level of troponin T does not exceed 0.2 - 0.5 ng / ml, so its increase above the specified limit indicates damage to the heart muscle.
The following laboratory tests are routinely performed in patients with suspected HF: general analysis blood(with the determination of the level of hemoglobin, the number of leukocytes and platelets), electrolyte analysis of blood, determination of serum creatinine and glomerular filtration rate (GFR), blood glucose, liver enzymes, urinalysis. Additional analyzes are performed depending on the specific clinical picture(Table 3).
Table 3- Typical laboratory abnormalities in patients with heart failure




Differential Diagnosis
Differential Diagnosis
Table 5 - Differential Diagnosis acute heart failure with other cardiological and non-cardiological diseases

Medical tourism
Get treatment in Korea, Israel, Germany, USA
Medical tourism
Get advice on medical tourism
Treatment
Treatment Goals
Purpose of emergency treatment- rapid stabilization of hemodynamics and reduction of symptoms (shortness of breath and / or weakness). Improvement in hemodynamic parameters, primarily CO and VR, PA and RA pressure.
Table 6- Treatment goals for AHF 
Treatment tactics
AHF is a life-threatening condition and requires urgent treatment. The following are interventions that are indicated for most patients with AHF. Some of them can be done quickly in any medical institution, others are available only to a limited number of patients and are usually carried out after initial clinical stabilization.
1) In AHF, the clinical situation requires urgent and effective interventions and can change quite quickly. Therefore, with rare exceptions (nitroglycerin under the tongue or nitrates in the form of an aerosol), drugs should be administered intravenously, which, in comparison with other methods, provides the most rapid, complete, predictable and manageable effect.
2) AHF leads to a progressive deterioration of blood oxygenation in the lungs, arterial hypoxemia and hypoxia of peripheral tissues. The most important task in the treatment of AHF is to ensure adequate tissue oxygenation to prevent their dysfunction and the development of multiple organ failure. To do this, it is extremely important to maintain the saturation of capillary blood within normal limits (95-100%).
oxygen therapy. In patients with hypoxemia, one should make sure that there is no impaired airway patency, then start oxygen therapy with an increased content of O2 in the respiratory mixture, which, if necessary, is increased. The feasibility of using increased concentrations of O2 in patients without hypoxemia is debatable: such an approach can be dangerous.
Respiratory support without endotracheal intubation (non-invasive ventilation). For respiratory support without tracheal intubation, two modes are mainly used: continuous positive airway pressure (CPAP) spontaneous breathing mode. The use of SPDS can restore lung function and increase functional residual volume. At the same time, lung compliance improves, the transdiaphragmatic pressure gradient decreases, and diaphragm activity decreases. All this reduces the work associated with breathing and reduces the metabolic needs of the body. The use of non-invasive methods in patients with cardiogenic pulmonary edema improves arterial blood pO2, reduces the symptoms of AHF, and can significantly reduce the need for tracheal intubation and mechanical ventilation.
Respiratory support with endotracheal intubation.
Invasive respiratory support (IVL with tracheal intubation) should not be used to treat hypoxemia that can be corrected by oxygen therapy and non-invasive ventilation methods.
Indications for mechanical ventilation with tracheal intubation are as follows:
Signs of weakness of the respiratory muscles - a decrease in the frequency of breathing in combination with an increase in hypercapnia and depression of consciousness;
Severe respiratory failure (in order to reduce the work of breathing);
The need to protect the respiratory tract from regurgitation of gastric contents;
Elimination of hypercapnia and hypoxemia in unconscious patients after prolonged resuscitation or drug administration;
The need for sanitation of the tracheobronchial tree to prevent atelectasis and bronchial obstruction.
The need for immediate invasive ventilation may occur with pulmonary edema associated with ACS.
3) It is necessary to normalize blood pressure and eliminate disorders that can cause a decrease in myocardial contractility (hypoxia, myocardial ischemia, hyper- or hypoglycemia, electrolyte disturbances, side effects or drug overdose, etc.). Attitude to the early introduction of special agents for the correction of acidosis (sodium bicarbonate, etc.) in last years quite restrained. The decreased response to catecholamines in metabolic acidosis has been questioned. Initially, it is more important to maintain adequate ventilation of the pulmonary alveoli and restore sufficient perfusion of peripheral tissues as soon as possible; further interventions may be required if hypotension and metabolic acidosis persist for a long time. To reduce the risk of iatrogenic alkalosis, it is recommended to avoid complete correction of the base deficiency.
4) In the presence of arterial hypotension, as well as before the appointment of vasodilators, it is necessary to make sure that there is no hypovolemia. Hypovolemia leads to insufficient filling of the chambers of the heart, which in itself is the cause of a decrease in cardiac output, arterial hypotension and shock. A sign that low BP is due to impaired heart pumping rather than insufficient filling is sufficient left ventricular filling pressure (pulmonary artery wedge pressure greater than 18 mmHg). When assessing the adequacy of filling the left ventricle in real clinical conditions, one often has to focus on indirect indicators(physical signs of congestion in the lungs, the degree of distension of the veins of the neck, data x-ray examination), however, they react rather late to favorable hemodynamic changes caused by treatment. The latter can lead to the use of unreasonably high doses of drugs.
5) An effective means to increase blood pressure, reduce left ventricular afterload and increase perfusion pressure in the coronary arteries is intra-aortic balloon counterpulsation (IBD). This improves the contractility of the left ventricle and reduces myocardial ischemia.
In addition, IBD is effective in the presence of mitral regurgitation and ventricular septal defects. It is contraindicated in aortic regurgitation, aortic dissection, and severe peripheral atherosclerosis. Unlike drug treatment, it does not increase myocardial oxygen demand (as positive inotropic agents), does not depress myocardial contractility, and does not reduce blood pressure (as drugs used to eliminate myocardial ischemia or reduce afterload). At the same time, this is a temporary measure that allows you to gain time in cases where it is possible to eliminate the causes of the developed condition (see below). In patients awaiting surgery, other means of mechanical support may be required (mechanical means of bypassing the left ventricle, etc.).
6) It is important to address the underlying causes of AHF in a particular patient. Eliminate tachycardia or bradycardia if they cause or exacerbate AHF.
If there are signs of an acute persistent occlusion of a large epicardial coronary artery (the appearance of persistent ST segment elevations on the ECG), it is necessary to restore its patency as soon as possible. There is evidence that in AHF, percutaneous angioplasty/stenting (possibly against the background of intravenous injection of platelet glycoprotein IIb/IIIa receptor blockers) or coronary artery bypass surgery (with corresponding coronary artery disease) is more effective than thrombolytic therapy, especially in the presence of cardiogenic shock.
In the presence of an exacerbation of coronary artery disease, when according to the ECG there are no signs of persistent occlusion of a large epicardial coronary artery (unstable angina, including postinfarction, acute myocardial infarction, not accompanied by ST segment elevations on the ECG), it is necessary to suppress myocardial ischemia as soon as possible and prevent it re-occurrence. The symptoms of AHF in such patients are an indication for the maximum possible antithrombotic treatment (including a combination acetylsalicylic acid, clopidogrel, heparin and, in some cases, intravenous infusion of a platelet glycoprotein IIb/IIIa receptor blocker) and to perform coronary angiography as soon as possible, followed by myocardial revascularization (the method depends on the coronary anatomy - percutaneous angioplasty / stenting or coronary artery bypass surgery). At the same time, angioplasty / stenting of the coronary arteries in early dates diseases should be carried out without stopping treatment with a combination of the above drugs. When rapid coronary artery bypass surgery is possible, it is suggested that clopidogrel be deferred pending coronary angiography results; if it turns out that the patient needs coronary bypass surgery and the operation is planned in the next 5-7 days, the drug should not be prescribed. If coronary artery bypass surgery can be performed within the next 24 hours, it is recommended to use unfractionated rather than low molecular weight heparin.
Perform the most complete myocardial revascularization in patients with chronic forms of coronary artery disease (especially effective in the presence of viable hibernated myocardium).
Perform surgical correction of intracardiac hemodynamic disorders ( valvular defects, atrial or ventricular septal defects, etc.); if necessary, quickly eliminate the tamponade of the heart.
In some patients, the only possible way treatment is a heart transplant.
However, complex invasive diagnostic and therapeutic interventions are not considered justified in patients with end-stage comorbidity, when AHF is based on an unrecoverable cause, or when corrective interventions or heart transplantation are not possible.
7) Diet of patients with AHF (after stabilization of the condition).
The main positions are as follows:
I functional class (FC) - do not eat salty foods (restriction of salt intake to 3 g NaCl per day);
II FC - do not add salt to food (up to 1.5 g of NaCl per day);
III FC - eat foods with a reduced salt content and cooking without salt (<1,0 г NaCl в день).
2. When limiting salt intake, limiting fluid intake is relevant only in extreme situations: with decompensated severe CHF, requiring intravenous diuretics. In normal situations, it is not recommended to use a fluid volume of more than 2 liters / day (maximum fluid intake is 1.5 liters / day).
3. Food should be high-calorie, easily digestible, with a sufficient content of vitamins and protein.
4. NB! Weight gain> 2 kg in 1-3 days may indicate fluid retention in the body and an increased risk of decompensation!
5. The presence of obesity or overweight worsens the patient's prognosis and in all cases with a body mass index (BMI) of more than 25 kg / m2 requires special measures and calorie restriction.
8) Mode physical activity bed
Physical rehabilitation contraindicated in:
active myocarditis;
Stenosis of valve openings;
cyanotic birth defects;
Violations of the rhythm of high gradations;
Attacks of angina pectoris in patients with low ejection fraction (EF), left ventricle (LV).
Drug treatment of chronic heart failure
essential medicines, used in the treatment of acute heart failure.
1) Positive inotropic agents temporarily used in AHF to increase myocardial contractility and their action is usually accompanied by an increase in myocardial oxygen demand.
Pressor (sympathomimetic) amines(norepinephrine, dopamine and, to a lesser extent, dobutamine), in addition to increasing myocardial contractility, can cause peripheral vasoconstriction, which, along with an increase in blood pressure, leads to a deterioration in oxygenation of peripheral tissues.
Treatment usually begins with small doses, which, if necessary, are gradually increased (titrated) until the optimal effect is obtained. In most cases, dose selection requires invasive monitoring of hemodynamic parameters with the determination of cardiac output and pulmonary artery wedge pressure. Common disadvantage drugs in this group is the ability to cause or aggravate tachycardia (or bradycardia when using norepinephrine), cardiac arrhythmias, myocardial ischemia, as well as nausea and vomiting. These effects are dose dependent and often preclude further dose increases.
Norepinephrine causes peripheral vasoconstriction (including celiac arterioles and renal vessels) due to stimulation of α-adrenergic receptors. In this case, cardiac output can either increase or decrease depending on the initial peripheral vascular resistance, the functional state of the left ventricle, and reflex influences mediated through carotid baroreceptors. It is indicated for patients with severe arterial hypotension (systolic blood pressure below 70 mm Hg), with low peripheral vascular resistance. The usual initial dose of norepinephrine is 0.5-1 mcg / min; in the future, it is titrated until the effect is achieved and in refractory shock it can be 8-30 mcg / min.
dopamine stimulates α- and β-adrenergic receptors, as well as dopaminergic receptors located in the vessels of the kidneys and mesentery. Its effect is dose dependent. With intravenous infusion at a dose of 2-4 mcg / kg per minute, the effect on dopaminergic receptors is mainly manifested, which leads to the expansion of celiac arterioles and renal vessels. Dopamine may help increase the rate of diuresis and overcome diuretic refractoriness caused by reduced renal perfusion, and can also affect renal tubules stimulating natriuresis. However, as noted, there is no improvement in glomerular filtration in patients with the oliguric stage of acute renal failure. In doses of 5-10 mcg / kg per minute, dopamine stimulates predominantly 1-adrenergic receptors, which contributes to an increase in cardiac output; venoconstriction is also noted. At doses of 10-20 mcg / kg per minute, stimulation of α-adrenergic receptors predominates, which leads to peripheral vasoconstriction (including celiac arterioles and renal vessels). Dopamine, alone or in combination with other pressor amines, is used to eliminate arterial hypotension, increase myocardial contractility, and increase heart rate in patients with bradycardia in need of correction. If dopmin administration at a rate of more than 20 mcg/kg/min is required to maintain blood pressure in a patient with sufficient ventricular filling pressure, it is recommended to add norepinephrine.
Dobutamine- synthetic catecholamine, stimulating mainly β-adrenergic receptors. In this case, there is an improvement in myocardial contractility with an increase in cardiac output and a decrease in the filling pressure of the ventricles of the heart. Due to a decrease in peripheral vascular resistance, blood pressure may not change. Since the goal of dobutamine treatment is to normalize cardiac output, monitoring of this indicator is required to select the optimal dose of the drug. Doses of 5-20 mcg/kg per minute are commonly used. Dobutamine can be combined with dopamine; it is able to reduce pulmonary vascular resistance and is the drug of choice in the treatment of right ventricular failure. However, already 12 hours after the start of the infusion of the drug, tachyphylaxis may develop.
Phosphodiesterase III inhibitors(amrinone, milrinone) have positive inotropic and vasodilating properties, causing predominantly venodilation and a decrease in pulmonary vascular tone. As well as pressor amines, they can aggravate myocardial ischemia and provoke ventricular arrhythmias. For their optimal use, monitoring of hemodynamic parameters is required; pulmonary artery wedge pressure should not be below 16-18 mm Hg. IV infusion of phosphodiesterase III inhibitors is usually used in severe heart failure or cardiogenic shock that does not adequately respond to standard treatment with pressor amines. Amrinon quite often causes thrombocytopenia, tachyphylaxis can quickly develop to it. It has recently been shown that the use of milrinone in worsening chronic heart failure does not lead to an improvement in the clinical course of the disease, but is accompanied by an increase in the incidence of persistent arterial hypotension requiring treatment and supraventricular arrhythmias.
Means that increase the affinity of contractile myofibrils of cardiomyocytes for calcium. The only drug in this group that has reached the stage of widespread clinical application in AHF, is levosimendan. Its positive inotropic effect is not accompanied by a noticeable increase in myocardial oxygen demand and an increase in sympathetic effects on the myocardium. Other possible mechanisms of action are selective inhibition of phosphodiesterase III, activation potassium channels. Levosimendan has a vasodilating and anti-ischemic effect; due to the presence of a long-acting active metabolite, the effect persists for some time after the drug is discontinued. Digoxin is of limited value in the treatment of AHF. The drug has a small therapeutic breadth and can cause severe ventricular arrhythmias, especially in the presence of hypokalemia. Its ability to slow atrioventricular conduction is used to reduce the frequency of ventricular contractions in patients with persistent atrial fibrillation or atrial flutter.
2) Vasodilators are able to quickly reduce pre- and afterload due to the expansion of veins and arterioles, which leads to a decrease in pressure in the capillaries of the lungs, a decrease in peripheral vascular resistance and blood pressure. They can not be used for arterial hypotension.
Isosorbide dinitrate peripheral vasodilator with a predominant effect on venous vessels. Antianginal agent. The mechanism of action is associated with the release of the active substance nitric oxide in the smooth muscles of the vessels. Nitric oxide activates guanylate cyclase and increases cGMP levels, which ultimately leads to smooth muscle relaxation. Under the influence of isosorbide dinitrate arterioles and precapillary sphincters
Relax to a lesser extent than large arteries and veins.
The action of isosorbide dinitrate is mainly associated with a decrease in myocardial oxygen demand due to a decrease in preload (dilation of peripheral veins and a decrease in blood flow to the right atrium) and afterload (decrease in peripheral vascular resistance), as well as with a direct coronary dilating effect. Promotes the redistribution of coronary blood flow in areas with reduced blood supply. Reduces pressure in the pulmonary circulation.
IV infusion usually begins with 10-20 micrograms / min and increases by 5-10 micrograms / min every 5-10 minutes until the desired hemodynamic or clinical effect is obtained. Low doses of the drug (30-40 mcg/min) mainly cause venodilation, higher doses (150-500 mcg/min) also lead to the expansion of arterioles. While maintaining a constant concentration of nitrates in the blood for more than 16-24 hours, tolerance develops to them. Nitrates are effective in myocardial ischemia, emergencies associated with arterial hypertension, or congestive heart failure (including mitral or aortic regurgitation). When using them, arterial hypotension should be avoided (its probability is increased with hypovolemia, lower localization of myocardial infarction, right ventricular failure). Hypotension caused by the use of nitrates is usually eliminated by intravenous fluid administration, the combination of bradycardia and hypotension is usually eliminated by atropine. They can also contribute to the onset or exacerbation of tachycardia, bradycardia, impaired ventilation-perfusion relationships in the lungs, and headache.
Nitrates are considered contraindicated in severe contractile dysfunction of the right ventricle, when its release depends on preload, with systolic blood pressure below 90 mm Hg, and also with a heart rate of less than 50 beats. per minute or severe tachycardia.
Sodium nitroprusside similar to nitroglycerin in its effect on arterioles and veins. It is usually administered in doses of 0.1-5 mcg/kg per minute (in some cases up to 10 mcg/kg per minute) and should not be exposed to light.
Used to treat emergencies arising from severe heart failure (especially associated with aortic or mitral regurgitation) and arterial hypertension. There is evidence of increased symptomatic efficacy (but not outcomes) in the treatment of conditions with low cardiac output and high peripheral resistance not responding to dopamine.
Sodium nitroprusside should not be used in persistent myocardial ischemia, as it can impair blood circulation in areas of blood supply to significantly stenotic epicardial coronary arteries. With hypovolemia, sodium nitroprusside, as well as nitrates, can cause a significant decrease in blood pressure with reflex tachycardia, so the filling pressure of the left ventricle should be at least 16-18 mm Hg.
Other side effects include exacerbation of hypoxemia in pulmonary disease (by eliminating hypoxic constriction of the pulmonary arterioles), headache, nausea, vomiting and abdominal cramps. With hepatic or renal insufficiency, as well as with the introduction of sodium nitroprusside at a dose of more than 3 μg / kg per minute for more than 72 hours, cyanide or thiocyanate may accumulate in the blood. Cyanide intoxication is manifested by the occurrence of metabolic acidosis. At concentrations of thiocyanate >12 mg/dL, lethargy, hyperreflexia, and convulsions occur.
Treatment consists in the immediate termination of the infusion of the drug, in severe cases, sodium thiosulfate is introduced.
3) Morphine- narcotic analgesic, which, in addition to analgesic, sedative action and an increase in vagal tone, causes venodilation.
It is considered as the drug of choice for the relief of pulmonary edema and the elimination of chest pain associated with myocardial ischemia and does not disappear after repeated sublingual nitroglycerin administration.
The main side effects include bradycardia, nausea and vomiting (eliminated by atropine), respiratory depression, and the occurrence or worsening of arterial hypotension in patients with hypovolemia (usually eliminated by elevating the legs and / in the introduction of fluid).
It is administered intravenously in small doses (10 mg of the drug is diluted in at least 10 ml physiological saline, administered intravenously slowly about 5 mg, then, if necessary, 2-4 mg at intervals of at least 5 minutes until the effect is achieved).
4) Furosemide- a loop diuretic with a direct venodilating effect. The latter effect occurs within the first 5 minutes after intravenous administration, while an increase in urine output occurs later.
The initial dose is 0.5-1 mg/kg IV. If necessary, the introduction is usually repeated after 1-4 hours.
5) Beta-blockers.
The use of drugs of this group in AHF associated with impaired myocardial contractility is contraindicated. However, in some cases, when pulmonary edema occurs in a patient with subaortic or isolated mitral stenosis and is associated with the occurrence of tachysystole, often in combination with elevated blood pressure, the introduction of a beta-blocker helps to relieve the symptoms of the disease.
Three drugs are available for intravenous use in Russia - propranolol, metoprolol and esmolol. The first two are administered in small doses at intervals sufficient to assess the efficacy and safety of the previous dose (changes in blood pressure, heart rate, intracardiac conduction, manifestations of AHF). Esmolol has a very short half-life (2-9 min), so in acute patients with high risk complications, its use is considered preferable.
6) Anticoagulants.
Anticoagulants are indicated for patients with ACS, atrial fibrillation, artificial heart valves, deep vein thrombosis lower extremities and TELA. There is evidence that subcutaneous administration of low molecular weight heparins (enoxaparin 40 mg 1 time / day, dalteparin 5000 ME 1 time / day) can reduce the incidence of deep vein thrombosis of the lower extremities in patients hospitalized with an acute therapeutic disease, incl. severe CH. Large studies comparing the prophylactic efficacy of low molecular weight heparins and unfractionated heparin (5000 IU s / c 2-3 times / day.) in AHF have not been conducted.
7) Fibrinolytic therapy.
Patients with ST-segment elevation MI and the possibility of PCI should undergo mechanical (catheter) reperfusion (primary coronary intervention) within 60 minutes from the moment of seeking help. In the absence of the possibility of primary PCI, restoration of blood flow in the infarct-dependent artery can be achieved by pharmacological reperfusion (fibrinolysis) within 30 minutes after the first contact with the patient.
Despite limited efficacy and a high risk of bleeding, fibrinolysis on prehospital stage should be considered as a priority method of treatment, in the presence of all conditions for its implementation (trained personnel with the ability to decipher the ECG). The bolus drug (tenecteplase) is easy to administer and has a better prognosis with less risk of bleeding.
In the absence of contraindications, it is necessary to start trobolytic therapy (TLT) under the following conditions:
If the time from the onset of an anginal attack is 4-6 hours, at least does not exceed 12 hours;
ECG shows ST-segment elevation >0.1 mV in at least 2 consecutive chest leads or 2 limb leads, or a new left bundle branch block (LBBB) appears.
The introduction of thrombolytics is justified at the same time with ECG signs of true posterior MI (high R waves in the right precordial leads V1-V2 and depression of the ST segment in leads V1-V4 with an upward T wave).
Recombinant tissue plasminogen activator (Alteplase) administered intravenously (previously the drug is dissolved in 100-200 ml of distilled water or 0.9% sodium chloride solution) according to the "bolus + infusion" scheme. Dose of the drug 1 mg / kg body weight (but not more than 100 mg): 15 mg is administered as a bolus; subsequent infusion of 0.75 mg / kg of body weight over 30 minutes (but not more than 50 mg), then 0.5 mg / kg (but not more than 35 mg) over 60 minutes (total duration of infusion - 1.5 hours).
Streptokinase administered in / in a dose of 1500000 ME for 30-60 minutes in a small amount of 0.9% sodium chloride solution. The development of hypotension, acute allergic reactions is often noted. Streptokinase should not be re-introduced (specify history) due to the appearance of antibodies that can affect its activity and the development of allergic reactions up to anaphylactic shock.
Tenecteplase (Metalise) intravenously 30 mg at body weight<60 кг, 35 мг при 60-70 кг, 40 мг при 70-80 кг; 45 мг при 80-90 кг и 50 мг при массе тела >90 kg, the required dose is given as a bolus over 5-10 seconds. For administration, a previously installed venous catheter can be used, but only if it is filled with a 0.9% sodium chloride solution, after the introduction of Metalise it must be well washed (in order to complete and timely delivery of the drug to the blood). Metalise is not compatible with dextrose solution, and should not be used with a dextrose drip. No other drugs should be added to the injection solution or to the infusion line. Considering more a long period half-life from the body, the drug is used as a single bolus, which is especially convenient in the treatment at the prehospital stage.
Absolute contraindications to fibrinolytic therapy:
Previous hemorrhagic stroke or disorder cerebral circulation unknown origin.
Ischemic stroke within the last 6 months, except for ischemic stroke occurring within 3 hours, which can be treated with thrombolytics.
Recent major trauma/surgery/injury to the head (within the last 3 months).
Brain tumor, primary or metastatic.
Changes in the structure of cerebral vessels, the presence of arteriovenous malformation, arterial aneurysms.
Suspicion of a dissecting aortic aneurysm.
Gastrointestinal bleeding within the past month.
The presence of signs of bleeding or hemorrhagic diathesis (with the exception of menstruation).
Punctures in places not giving in to compression (for example, liver biopsy, lumbar puncture).
Relative contraindications to fibrinolytic therapy:
Transient ischemic attack in the last 6 months.
Refractory arterial hypertension (systolic blood pressure ≥180 mm Hg and / or diastolic blood pressure ≥110 mm Hg).
Taking indirect anticoagulants (warfarin) (the higher the INR, the higher the risk of bleeding).
The state of pregnancy or within 1 week after childbirth.
Liver disease in an advanced stage.
Aggravation peptic ulcer or 12 duodenal ulcer.
Infective endocarditis.
Ineffective resuscitation measures. Traumatic or prolonged (> 10 min) cardiopulmonary resuscitation.
For streptokinase, prior use (> 5 days ago and up to one year or more) or allergic reaction on her.
The criteria for a successful fibrinolysis are a decrease in ST segment shift on the ECG by more than 50% within 60-90 minutes (should be documented in the medical history), the occurrence of typical reperfusion arrhythmias, and the disappearance of chest pain.
Features of the treatment of AHF depending on the cause of decompensation
Elimination of the cause of decompensation is an essential component of the treatment of AHF and the prevention of its recurrence. Non-cardiac diseases can seriously complicate the course of AHF and make it difficult to treat.
ischemic heart disease
It is the most common cause of AHF, which can be represented by left ventricular failure with low CO, left ventricular failure with symptoms of blood stasis, and right ventricular failure. All patients with exacerbation of coronary artery disease are shown to perform CAG as soon as possible.
Timely reperfusion in AMI with ST elevations on the ECG can prevent AHF or improve its course. Percutaneous coronary intervention is preferred, and emergency coronary bypass surgery is warranted in patients with cardiogenic shock if indicated. If invasive treatment is not available or is associated with a significant loss of time, TLT should be performed. Urgent myocardial revascularization is also indicated for AHF, complicating myocardial infarction, without ST segment elevations on the ECG. as well as in NS with severe myocardial ischemia.
The occurrence of AHF during exacerbation of coronary artery disease can contribute to reflex reactions, as well as disturbances in the heart rhythm and conduction. Therefore, both adequate pain relief and fast elimination arrhythmias leading to hemodynamic disturbances.
In true cardiogenic shock, temporary stabilization can be achieved by maintaining adequate filling of the heart chambers, VACP, medical inotropic support, and mechanical ventilation. For left ventricular failure with symptoms of blood stasis, acute treatment is the same as for other causes of this variant of AHF. Because inotropic agents can be hazardous, the possibility of UACP should be discussed. Subsequently, along with adequate myocardial revascularization, β-blockers and RAAS inhibitors are indicated.
More detailed approaches to the treatment of AHF during exacerbation of coronary artery disease are set out in the recommendations of the VNOK for the treatment of myocardial infarction with ST segment elevations on the ECG and ACS without persistent ST segment elevations on the ECG (Kardiology. - 2004. - No. 4 (appendix). - P. 1-28 ).
Pathology of the valvular apparatus of the heart
The cause of AHF can be dysfunction of the heart valves during exacerbation of coronary artery disease (often mitral insufficiency), acute mitral or aortic insufficiency of another etiology (endocarditis, trauma), aortic or mitral stenosis, artificial valve thrombosis, exfoliating aortic aneurysm.
At infective endocarditis The main cause of AHF is heart valve insufficiency. The severity of cardiac dysfunction may be exacerbated by myocarditis. Antibiotics should be given in addition to standard treatment for AHF. For a quick diagnosis, a specialist consultation is indicated.
With severe acute mitral or aortic insufficiency, urgent surgical treatment is required. With long-term mitral regurgitation in combination with reduced CI and low EF, emergency surgery usually does not improve the prognosis. In these cases great importance may have a preliminary stabilization of the state with the help of UACP.
Thrombosis of the artificial heart valve
AHF in these patients often leads to death. In all patients with suspected prosthetic valve thrombosis, chest x-ray and echocardiography should be performed. question about optimal treatment remains unclear. In left heart valve thrombosis, surgery is the treatment of choice. TLT is used for right heart valve thrombosis and in cases where surgery is associated with a high risk.
For TLT, a recombinant inhibitor of tissue plasminogen activator (10 mg IV by bolus followed by an infusion of 90 mg over 90 minutes) and streptokinase (250,000-500,000 IU over 20 minutes followed by an infusion of 1,000,000-1.5,000,000 ME for 10 hours). After the introduction of a thrombolytic, it is necessary to start an IV infusion of unfractionated heparin at a dose that provides an increase in APTT by 1.5-2 times from the normal (control) values for this laboratory. Alternatives include urokinase 4400 IU/(kg h) without heparin for 12 h or 2000 IU/(kg h) plus unfractionated heparin for 24 h.
TLT is ineffective if there is an overgrowth of fibrous tissue with small areas of secondary thrombosis. In patients with very large and/or mobile thrombi, TLT is associated with increased risk thromboembolic complications and stroke. In these cases, surgical treatment is possible. Preliminarily, to clarify the nature of the valve lesion, transesophageal echocardiography was indicated. After TLT, a repeat echocardiogram is necessary. The expediency of surgical intervention should be considered if TLT is unable to eliminate occlusion.
An alternative method is to administer additional doses of thrombolytic. Although mortality during emergency surgery in patients with hemodynamic instability of III-IV FC, according to the classification of the New York Heart Association (NYHA) (pulmonary edema, arterial hypotension), is high, TLT can lead to loss of time and further increase the risk of surgical treatment in case of her failure. According to non-randomized trials, in less severe patients, long-term antithrombotic and/or TLT may be as effective as surgical treatment.
Dissecting aortic aneurysm
Dissecting aortic aneurysm is accompanied by AHF in the presence of GC, acute valvular regurgitation, cardiac tamponade, myocardial ischemia. If a dissecting aortic aneurysm is suspected, an emergency consultation with a surgeon is necessary. The morphology and function of the aortic valve, as well as the presence of fluid in the pericardium, are best assessed by transesophageal echocardiography. Surgical intervention is usually performed according to vital indications.
Cardiac tamponade
Cardiac tamponade is a decompensated phase of its compression caused by the accumulation of fluid in the pericardium. With "surgical" tamponade (bleeding), intrapericardial pressure increases rapidly - from several minutes to hours, while with "therapeutic" tamponade (inflammation), this process takes from several days to weeks. Violation of hemodynamics - absolute reading to pericardiocentesis. In patients with hypovolaemia, temporary improvement can be achieved by intravenous fluid administration, leading to an increase in the filling pressure of the ventricles of the heart.
In case of wounds, rupture of an aneurysm of the ventricle of the heart or hemopericardium due to aortic dissection, surgery is necessary to eliminate the source of bleeding. Whenever possible, the cause of effusion pericarditis should be treated.
OSN is one of the most frequent complications hypertensive crises.
Clinical signs AHF in hypertensive crisis includes only congestion in the lungs, which can be minor or severe, up to sudden pulmonary edema.
Patients hospitalized with pulmonary edema on the background of a hypertensive crisis often do not find significant changes in LV systolic function; more than half of LV EF > 45%. Diastolic disturbances are often observed, in which the processes of relaxation of the myocardium worsen.
The goal of the treatment of acute pulmonary edema against the background of hypertension is to reduce pre- and afterload on the left ventricle, myocardial ischemia and eliminate hypoxemia by maintaining adequate ventilation of the lungs. Treatment should begin immediately in the following order: oxygen therapy, PPD or other non-invasive ventilation regimens, if necessary - mechanical ventilation, usually on short period, in combination with the / in the introduction of antihypertensive drugs.
Antihypertensive therapy should cause a fairly rapid, within a few minutes, decrease in SBP or DBP by 30 mm Hg. Subsequently, a slower decrease in blood pressure to the values that occurred before the hypertensive crisis is shown, usually within a few hours. Do not try to lower blood pressure to normal levels, as this may lead to a decrease in organ perfusion. An initial rapid decrease in blood pressure can be achieved by prescribing the following drugs, either alone or in combination (while maintaining hypertension):
In / in the introduction of isosorbide dinitrate, nitroglycerin or nitroprusside;
In / in the introduction of loop diuretics, especially in patients with fluid retention and a long history of CHF;
Perhaps in / in the introduction of a long-acting derivative of dihydropyridine (nicardipine). However, with a hemodynamic effect similar to nitrates, drugs of this group can cause hypersympathicotonia (tachycardia), increase blood shunting in the lungs (hypoxemia), and also give complications from the central nervous system.
A rapid decrease in blood pressure can be achieved by taking captopril under the tongue. Apparently, its use can be justified if it is impossible to administer drugs intravenously, as well as the inaccessibility or insufficient effectiveness of inhaled forms of nitrates.
β-Adrenergic blockers should not be used for pulmonary edema, unless AHF is combined with tachycardia in patients without a serious impairment of LV contractility, for example, with diastolic HF, mitral stenosis. Hypertensive crisis in pheochromocytoma can be eliminated by intravenous administration of 5-15 mg of phentolamine with mandatory monitoring of blood pressure; re-introduction is possible after 1-2 hours.
kidney failure
Minor and moderate change kidney function is usually asymptomatic and satisfactorily tolerated by patients, however, even a slightly elevated serum creatinine and/or a decrease in GFR are independent risk factors for poor prognosis in AHF.
In the presence of acute renal failure, diagnosis and treatment of comorbidities are necessary: anemia, electrolyte disturbances and metabolic acidosis. Renal failure affects the effectiveness of HF therapy, which involves the use of digoxin, ACE inhibitors, angiotensin receptor blockers, spironolactone. An increase in serum creatinine by more than 25-30% and / or reaching a concentration exceeding 3.5 mg / dL (266 μmol / L) is a relative contraindication to continuing ACE inhibitor therapy.
Moderate to severe renal failure [serum creatinine greater than 2.5–3 mg/dL (190–226 µmol/L)] is associated with decreased response to diuretics. These patients often need constant increase doses of loop diuretics and/or in the addition of a diuretic with a different mechanism of action. This, in turn, can cause hypokalemia and further decrease in GFR. The exception is torasemide, the pharmacological properties of which practically do not depend on impaired renal function, since the drug is metabolized by 80% in the liver.
Sick with severe dysfunction kidneys and refractory fluid retention may require continuous veno-venous hemofiltration.
The combination with inotropic agents enhances renal blood flow, improves kidney function, and restores the effectiveness of diuretics. Hyponatremia, acidosis, and uncontrolled fluid retention may require dialysis. The choice between peritoneal dialysis, hemodialysis and ultrafiltration usually depends on the technical equipment of the hospital and the value of blood pressure.
Lung disease and bronchial obstruction
When ASI is combined with broncho-obstructive syndrome, it is necessary to use bronchodilators. Although this group of drugs may improve heart function, they should not be used to treat AHF.
Albuterol is usually used (0.5 ml of a 0.5% solution in 2.5 ml of saline through a nebulizer for 20 minutes). The procedure can be repeated every hour for the first few hours, and in the future - according to indications.
Heart rhythm disorders
Heart rhythm disturbances can be the main cause of AHF in patients with both preserved and impaired heart function, as well as complicate the course of already developed AHF. To prevent and successfully eliminate heart rhythm disturbances, it is necessary to maintain a normal concentration of potassium and magnesium in the blood.
Bradyarrhythmias
Treatment usually begins with intravenous administration of 0.25-5 mg of atropine, if necessary, repeatedly up to a maximum dose of 2 mg. With atrioventricular dissociation with rare ventricular activity in patients without myocardial ischemia, an intravenous infusion of isoproterenol at a dose of 2-20 mcg / min can be used.
Low heart rate in atrial fibrillation can be temporarily eliminated by intravenous administration of theophylline at a rate of 0.2-0.4 mg / (kg h), first as a bolus, then as an infusion. If there is no response to medical treatment, an artificial pacemaker should be used. In the presence of myocardial ischemia, it should be eliminated as soon as possible.
Supraventricular tachyarrhythmias
Atrial fibrillation and atrial flutter. It is necessary to control the heart rate, especially in the presence of diastolic myocardial dysfunction. However, in restrictive HF or cardiac tamponade, with a rapid decrease in heart rate, the condition of patients may suddenly worsen.
Depending on the clinical situation, it is possible to maintain normosystole with persistent arrhythmia or recovery and retention sinus rhythm. If the arrhythmias are paroxysmal, medical or electrical cardioversion should be considered once the condition has stabilized. With a duration of paroxysm of less than 48 hours, the use of anticoagulants is not necessary.
Table 7. - Treatment of arrhythmias in AHF 
If the arrhythmia persists for more than 48 hours, anticoagulants should be used and for at least three weeks before cardioversion, maintain normosystole with appropriate medicines. In more severe cases: arterial hypotension, severe pulmonary congestion - urgent electrical cardioversion is indicated against the background of the introduction of a therapeutic dose of heparin. The duration of anticoagulant use after successful cardioversion should be at least 4 weeks. In patients with persistent atrial fibrillation and atrial flutter, the advisability of using anticoagulants depends on the degree of risk of arterial thromboembolism and is considered in the relevant guidelines.
β-blockers are used to reduce heart rate and prevent recurrence of arrhythmia. Rapid digitalization should also be considered, especially when atrial fibrillation is secondary to AHF. Amiodarone is commonly used for medical cardioversion and prevention of arrhythmia recurrence.
Patients with low EF should not use antiarrhythmic drugs class I, verapamil and diltiazem. In rare cases, the possibility of prescribing verapamil can be considered in patients without a significant decrease in LV contractility to control heart rate or eliminate paroxysmal supraventricular tachycardia with narrow QRS complexes.
ventricular arrhythmias.
Ventricular fibrillation and sustained ventricular tachycardia require immediate EIT and, if necessary, respiratory support.
Amiodarone and β-blockers can prevent their recurrence.
In case of recurrence of severe ventricular arrhythmias and hemodynamic instability, CAG and electrophysiological studies should be performed immediately.
Other types of treatment:- as a treatment option, after the transition to the terminal stage of CHF, this is the implantation of mechanical assistive devices to support the left ventricle, as well as heart transplantation (for details, see CHF treatment).
Surgical intervention
1) Emergency coronary angiography should be performed as soon as possible in patients with severe angina, profound or dynamic ECG changes, severe arrhythmias, or hemodynamic instability on admission or thereafter. These patients make up 2-15% of patients admitted with a diagnosis of ST ACS.
Patients at high thrombotic risk and at high risk for developing myocardial infarction should undergo angiographic examination without delay. Especially in the presence of clinical symptoms of HF or progressive hemodynamic instability (shock) and life-threatening cardiac arrhythmias (VF-ventricular fibrillation, VT-ventricular tachycardia) (Table 8).
Table 8- Predictors of high thrombotic risk or high risk of myocardial infarction, which are an indication for urgent coronary angiography 
Patients with persistent symptoms of ischemia and signs of ST segment depression in the anterior chest leads (particularly in combination with an increase in troponin), which may indicate probable posterior transmural ischemia, should undergo emergency coronary angiography (<2 ч).
Patients with persistent symptoms or documented troponin elevation, in the absence of diagnostic ECG changes, also require emergency coronary angiography to identify acute thrombotic occlusion in the left circumflex artery. Especially in cases where the differential diagnosis of another clinical situation remains unclear.
2) Surgical treatment. For some of the underlying conditions of AHF, prompt surgical intervention can improve prognosis (Table 9). Surgical methods of treatment include myocardial revascularization, correction of anatomical defects of the heart, including valve replacement and reconstruction, mechanical means of temporary blood circulation support. The most important diagnostic method in determining indications for surgery is echocardiography.
Table 9- Heart disease in AHF requiring surgical correction 
3) Heart transplantation. The need for heart transplantation usually occurs with severe acute myocarditis, postpartum cardiomyopathy, extensive MI with a poor prognosis after revascularization.
Heart transplantation is not possible until the patient is stabilized with mechanical circulatory support.
4) Mechanical ways to support blood circulation. Temporary mechanical circulatory support is indicated for patients with AHF who do not respond to standard treatment, when it is possible to restore myocardial function, surgical correction of existing disorders with a significant improvement in heart function or heart transplantation is indicated.
Levitronix devices- refers to devices that provide hemodynamic support (from several days to several months), with minimal trauma to blood cells. Without oxygenation.
Intra-aortic balloon counterpulsation (IACP)
The standard component of the treatment of patients with cardiogenic shock or severe acute LV insufficiency in the following cases:
- lack of rapid response to fluid administration, treatment with vasodilators and inotropic support;
- severe mitral regurgitation or rupture of the interventricular septum to stabilize hemodynamics, allowing you to perform the necessary diagnostic and therapeutic measures;
- severe myocardial ischemia (as a preparation for CAG and revascularization).
VACP can significantly improve hemodynamics, but it should be performed when it is possible to eliminate the cause of AHF - myocardial revascularization, heart valve replacement or heart transplantation, or its manifestations can regress spontaneously - myocardial stunning after AMI, open heart surgery, myocarditis.
VACP is contraindicated in aortic dissection, severe aortic insufficiency, severe peripheral arterial disease, fatal causes of heart failure, and multiple organ failure.
Extracorporeal membrane oxygenation (ECMO)
ECMO - the use of mechanical devices for temporary (from several days to several months) support of the function of the heart and / or lungs (in whole or in part) in cardiopulmonary insufficiency, which leads to the restoration of organ function or its replacement
Indication for ECMO in heart failure in adults - cardiogenic shock:
- Insufficient tissue perfusion manifesting as hypotension and low cardiac output despite adequate volemia
- Shock persists despite administration of volume, inotropes, and vasoconstrictors, and intra-aortic balloon pump if needed
Implantation of VAD assistive devices:
The use of these devices in the treatment of severe heart failure is considered in two aspects. The first is a "bridge" to heart transplantation (bridge to transplantation), i.e. the device is used temporarily while the patient waits for a donor heart. The second is a "bridge" to recovery, when, thanks to the use of an artificial heart ventricle, the function of the heart muscle is restored.
5) Ultrafiltration
Venovenous isolated ultrafiltration is sometimes used to remove fluid in patients with HF, although it is usually used as a reserve therapy for diuretic resistance.
Preventive actions:
The basis of emergency cardiology should be the active prevention of emergency cardiac conditions.
Three areas of prevention of emergency cardiac conditions can be distinguished:
- primary prevention of cardiovascular diseases;
- secondary prevention in existing cardiovascular diseases;
- urgent prevention in case of exacerbation of the course of cardiovascular diseases.
Emergency Prevention- a set of emergency measures to prevent the occurrence of an emergency cardiological condition or its complications.
Emergency prevention includes:
1) immediate measures to prevent the development of an emergency cardiac condition with a sharp increase in the risk of its occurrence (when the course of cardiovascular disease worsens, anemia, hypoxia; before the inevitable high physical, emotional or hemodynamic load, surgery, etc.);
2) a set of self-help measures used by patients with cardiovascular diseases in the event of an emergency within the framework of an individual program previously developed by a doctor;
3) the earliest possible and minimally sufficient emergency medical care;
4) additional measures to prevent the development of complications of emergency cardiac conditions.
The development by the attending physician of individual self-help programs for patients with cardiovascular diseases can bring significant benefits.
The basis of emergency cardiac care is the elementary organization and equipment of the treatment and diagnostic process, and most importantly, specialists with clinical thinking, practical experience and dedication.
Indicators of treatment efficacy and safety of diagnostic and treatment methods described in the protocol
Criteria for the effectiveness of treatment of patients with AHF:
Evaluation of the effectiveness of treatment of AHF:
1. achieving symptomatic improvement;
2. survival of patients after AHF in the long term;
3. increase in life expectancy.
Drugs (active substances) used in the treatment
| Adenosine |
| Alteplase (Alteplase) |
| Amiodarone (Amiodarone) |
| Amrinone (Amrinone) |
| Atropine (Atropine) |
| Vasopressin for injections (Vasopressin injection) |
| Heparin sodium (Heparin sodium) |
| Dalteparin (Dalteparin) |
| Digoxin (Digoxin) |
| Dobutamine (Dobutamine) |
| Dopamine (Dopamine) |
| Isoproterenol |
| Isosorbide dinitrate (Isosorbide dinitrate) |
| Captopril (Captopril) |
| Levosimendan (Levosimendan) |
| Lidocaine (Lidocaine) |
| Metoprolol (Metoprolol) |
| Milrinone (Milrinone) |
| Morphine (Morphine) |
| Sodium nitroprusside (Sodium nitroprusside) |
| Nicardipine (Nicardipine) |
| Nitroglycerin (Nitroglycerine) |
| Norepinephrine (Norepinephrine) |
| Propranolol (Propranolol) |
| Salbutamol (Salbutamol) |
| Streptokinase (Streptokinase) |
| Tenecteplase (Tenecteplase) |
| Theophylline (Theophylline) |
| Torasemide (Torasemide) |
| Urokinase (Urokinase) |
| Phentolamine (Phentolamine) |
| Furosemide (Furosemide) |
| Enoxaparin sodium (Enoxaparin sodium) |
| Epinephrine (Epinephrine) |
| Esmolol (Esmolol) |
Groups of drugs according to ATC used in the treatment
| (C03C) Loop diuretics |
| (C07) Beta blockers |
| (C09) Drugs affecting the renin-angiotensin system |
| (J01) Antimicrobials for systemic use |
- Pathogenesis of acute heart failure (left ventricular form)
- Pathogenesis of acute heart failure (right ventricular variety)
- Primary and secondary causes of acute heart failure
- Acute heart failure: causes and classification
Due to circulatory disorders in the heart develops, the reasons why it can occur are quite extensive. From a medical point of view, acute heart failure is not regarded as a disease - it is a consequence of past illnesses.
The heart is not able to pump the volume of blood that is necessary for the balanced functioning of the whole organism. It should be noted that almost every disease of the cardiovascular system can cause this syndrome. Acute insufficiency can also occur due to frequent nervous overstrain, may be the result of constant stressful situations or depression. 82% of overweight people suffer from heart failure.
Pathogenesis of acute heart failure (left ventricular form)
This type is much more common than the right ventricular form. Due to the influence of various factors, the contractility of the left ventricle decreases, and the function of the right ventricle can be preserved.
 In this case, the pulmonary vessels overflow with blood, respectively, there is an increase in pressure in the arteries (the pulmonary circulation), which gives rise to the process of plasma leakage through the walls of the vessels. Due to pathological changes, gas exchange is disturbed, the balance of oxygen in the blood, tissues, and, as a result, respiratory failure appears. Accordingly, a large number of substances such as:
In this case, the pulmonary vessels overflow with blood, respectively, there is an increase in pressure in the arteries (the pulmonary circulation), which gives rise to the process of plasma leakage through the walls of the vessels. Due to pathological changes, gas exchange is disturbed, the balance of oxygen in the blood, tissues, and, as a result, respiratory failure appears. Accordingly, a large number of substances such as:
- adrenalin;
- norepinephrine;
- biologically active substances.
All these processes lead to the fact that the vessels become permeable, peripheral resistance increases, and this is a direct path to pulmonary edema.
Back to index
Pathogenesis of acute heart failure (right ventricular variety)
 Right ventricular acute heart failure can develop when there is an excess flow of fluid, that is, the ventricle is simply overloaded. The reasons for this may be thromboembolism, embolism, rapid transfusion of blood, replacing blood fluids. Especially in cases where the catheter is inserted into the subclavian or jugular vein.
Right ventricular acute heart failure can develop when there is an excess flow of fluid, that is, the ventricle is simply overloaded. The reasons for this may be thromboembolism, embolism, rapid transfusion of blood, replacing blood fluids. Especially in cases where the catheter is inserted into the subclavian or jugular vein.
The thromboembolic form can occur with the formation of blood clots in the veins of the legs (varicose veins), attacks of atrial fibrillation, smoking, prolonged standing in one position, increased blood clotting. All of these processes cause an increase in blood viscosity and the formation of blood clots, which interfere with normal blood flow and contribute to overloading the right ventricle.
Back to index
Primary and secondary causes of acute heart failure
One of the main and main causes of the development of the disease is impaired contractile function of the myocardium. The causes of occurrence can be classified into two groups: they can be primary or secondary. But such a classification can be called conditional. Almost always, acute insufficiency is formed due to a mixed type of causes.
The primary causes of the development of the disease are: acute infectious diseases, exposure to the body of toxic poisons when poisoned by them.
 It is not for nothing that doctors believe that infectious diseases cannot be carried “on their feet”, because they give a complication to the heart. Some of the primary causes of acute deficiency are the consequences of influenza, rheumatism, measles, childhood scarlet fever, hepatitis, typhoid fever, acute respiratory viral infections, especially in severe cases and the occurrence of sepsis. All of these diseases contribute to the formation of acute inflammation, which, in turn, leads to the development of cell dystrophy, oxygen exchange is disturbed and hypoxia (oxygen starvation) occurs, there is a lack of nutrients in cells and tissues. Disturbed nervous regulation affects the heart muscle, which leads to a deterioration in its condition or dystrophy. The causes of acute deficiency can be severe strokes, their consequences, renal pathologies, alcohol, nicotine, drugs and drugs (especially in case of overdose), anemia, diabetes mellitus.
It is not for nothing that doctors believe that infectious diseases cannot be carried “on their feet”, because they give a complication to the heart. Some of the primary causes of acute deficiency are the consequences of influenza, rheumatism, measles, childhood scarlet fever, hepatitis, typhoid fever, acute respiratory viral infections, especially in severe cases and the occurrence of sepsis. All of these diseases contribute to the formation of acute inflammation, which, in turn, leads to the development of cell dystrophy, oxygen exchange is disturbed and hypoxia (oxygen starvation) occurs, there is a lack of nutrients in cells and tissues. Disturbed nervous regulation affects the heart muscle, which leads to a deterioration in its condition or dystrophy. The causes of acute deficiency can be severe strokes, their consequences, renal pathologies, alcohol, nicotine, drugs and drugs (especially in case of overdose), anemia, diabetes mellitus.
Secondary ones do not have a direct effect on the myocardium. That is, it occurs due to overwork and oxygen starvation. Such disorders can occur against the background of a hypertensive crisis, tachycardia, arrhythmia (paroxysmal diseases that are associated with an imbalance in the rhythm), atherosclerotic damage to the coronary vessels. The cause of acute heart failure can be the herpes virus, cytomegalovirus, which damage the coronary vessels.
If a person, for example, has hypertension, then the heart muscle works with increased vascular resistance. The myocardium increases in size - its thickness reaches 3 cm, although normally it should be no more than 14 mm. The mass of the heart also increases to 0.5 kg (the norm is 385 g). It is very difficult for the vessels to supply the necessary volume of blood to the enlarged heart muscle. Due to the fact that there is a pathological change and a violation of the ability to contract, with an attack of hypertension, heart failure occurs.
Back to index
Acute heart failure: causes and classification
 The causes of this disease can be classified by dividing them into the following groups:
The causes of this disease can be classified by dividing them into the following groups:
- on which myocardial damage occurs;
- on which the heart is overloaded;
- causing disruption of rhythms;
- which cause the heart to overflow with blood.
Acute heart failure can occur when the causes are destructive and myocardial damage occurs. This can happen against the background of myocarditis (infectious inflammation of the muscle), cardiomyopathy (myocardial damage caused by non-inflammatory processes and tumors), myocardial infarction (thrombosis of the coronary artery), angina pectoris (a form of coronary disease), cardiosclerosis (damage to valves and muscles due to the development scar tissue in them). Allergic tissue damage caused by bronchial asthma, Lyell's syndrome can cause myocardial destruction. In systemic connective tissue diseases (against the background of lupus or rheumatism), acute circulatory failure may develop.
It can also occur due to cardiac overload. In such cases, the heart pumps either large volumes of blood, or works with a large resistance of blood vessels. Acute insufficiency during overload may appear as a result of stenosis of the aorta or pulmonary trunk (a barrier is created to the exit of blood flow from the heart), arterial hypertension (increased pressure in the arteries), pulmonary hypertension (dramatically increased intravascular pressure in the blood flow of the pulmonary arteries), pathological changes in the valve apparatus ( develops with congenital and acquired defects).
 Impaired heart rate can be considered the cause of acute heart failure. Failure of the heart rate occurs if the electrolyte balance, urea and creatinine levels are disturbed, so the contractions simply become ineffective. The reason for the failure of rhythms can be atrial fibrillation, tachycardia, bradyarrhythmia.
Impaired heart rate can be considered the cause of acute heart failure. Failure of the heart rate occurs if the electrolyte balance, urea and creatinine levels are disturbed, so the contractions simply become ineffective. The reason for the failure of rhythms can be atrial fibrillation, tachycardia, bradyarrhythmia.
Acute failure can occur as a result of an altered process of filling the heart with blood. The etiology lies in the external compression of the heart walls or because of their rigidity. Such obstacles do not allow filling the heart with sufficient volume of blood, which leads to pathological changes in blood pumping and circulation in general. The causes of acute failure with such pathological changes are pericarditis (inflammation of the outer protective shell of the heart - the pericardium), cardiac tamponade (pathological changes in cardiac hypodynamics). Heart failure develops from stenosis of the atrioventricular valves (narrowing of the atrioventricular orifice), amyloidosis, fibroelastosis (increased stiffness of the walls of the heart).
In childhood (up to 3 years), the causes of acute insufficiency can be: congenital heart disease, myocarditis, complications after infectious diseases. In adolescents, acute heart failure occurs more often due to the use of drugs and smoking.
It is necessary to treat acute heart failure only in stationary conditions, in no case should you self-medicate, the disease can provoke the accumulation of fluid in the respiratory tract, slow down blood flow, which will lead to brain hypoxia, kidney dysfunction. In many cases, if neglected, acute heart failure causes death.
Acute heart failure (ICD code 150) is a decrease in the efficiency of the heartbeat. The mechanism of the development of pathology can be briefly described as follows: in the lungs and heart, blood circulation is disturbed, from which the myocardium is overloaded, which leads to its inability to fully pump blood. The pathogenesis of AHF is diverse, the classification of acute heart failure implies a previous chronic course (CHF may be a consequence of already present cardiac pathologies), or acute. Most often, the disease is a complication after a myocardial infarction. This syndrome can overtake both in the elderly and at a young age.
The causes of acute heart failure in both women and men are divided into primary and secondary, but more often cardiologists are faced with a mixed type of disorders.
The primary causes of pathology in adults and children may include:
- Acute infectious diseases: hepatitis, influenza, scarlet fever in children, measles, typhoid fever, rheumatism.
- Toxin poisoning, for example, carbon monoxide, chlorine, carbon monoxide, methyl alcohol.
- Food poisoning in children and adults.
From these pathologies, the cells of the heart muscles become inflamed or their dystrophy occurs. Nutrition and the necessary substances are supplied in smaller quantities, nervous regulation is disturbed, and the condition of the heart muscle becomes worse.
Secondary causes of the disease do not have a direct effect on the myocardium, but lead to general fatigue and lack of oxygen. These deviations include:
- Paroxysmal arrhythmias.
- Hypertensive crisis.
- Severe atherosclerotic damage to the coronary vessels.
With hypertension, the heart increases in weight, the vessels supply it poorly, contractility is disturbed, which leads to an acute form of the disease. Atherosclerotic plaques create prerequisites for oxygen deficiency, preventing sufficient blood flow to the heart. Acute heart failure is a phenomenon in which myocardial cells generally cease to participate in the blood circulation process, causing hypoxia.
Congenital heart anomalies, myocarditis, and acute infections can often cause heart failure in children under three years of age. Later, the syndrome of acute heart failure in a child often develops due to the effect on the heart of severe poisoning. The danger is that in children, symptoms appear only after a while.
How to recognize the disease
Depending on which part of the heart is overloaded, the disease is divided into right ventricular and left ventricular varieties. Signs of both types of acute heart failure differ from each other.
Manifestations of pathology of the left ventricle occur in the following cases:
- Left ventricular infarction.
- Hypertensive crisis.
- Violations of the rhythm of the heartbeat.
- Poor performance of the aortic valves.
The acute left ventricular form of the disease is often called cardiac asthma. With this disease, seizures occur (more often at night) associated with shortness of breath. Symptoms of this type of pathology include:

- shortness of breath
- inability to take a lying position;
- lack of air, the unreality of taking a deep breath;
- pallor;
- almost blue lips;
- cough with sputum in the form of foam;
- wheezing breathing;
- reduced pressure in the arteries;
- pain behind the chest, which is difficult to relieve;
- increasing general circulatory disorders.
If you do not provide the patient with timely medical care, this condition can cause pulmonary edema, the signs of which are considered bubbling breaths. Then the rhythm of breathing changes, until it stops completely. The most severe sign of left ventricular disability is cardiogenic shock and collapse. It happens if about half of the myocardium suddenly stops contracting. This condition is life threatening.
Symptoms appear in the following conditions:
- Right ventricular infarction.
- Pericarditis (during the compression of the right side of the heart).
- Difficult uncontrolled seizure in bronchial asthma.
- Thromboembolism of the artery of the lung.
During the right ventricular type, the following symptoms are noted:
- Acute pain sensations under the right hypochondrium (from the fact that there is an extra volume of blood in the liver).
- Swollen veins in the neck (visible in children).
- Significant overload of the right ventricle (this can be seen on the ECG).

Acute heart failure is a condition in which it is possible to help the patient only in a hospital setting.
Symptoms before death
The death of a patient with an acute form of pathology is often described as an accident, occurs outside the hospital walls and can occur from overexertion (both physical and nervous). Half of the patients, shortly before the moment of death, expressed near-death complaints of burning pressing pain in the heart and a feeling of fear.
In a quarter of patients, death occurs instantly against the background of a stable condition, in the rest, a couple of weeks before death, early manifestations of an impending catastrophe are noted, such as:
- More frequent heart pain.
- General weakness.
- Dyspnea.
- Increased fatigue.
- Inability to cope with physical stress.
- Arrhythmia.
Weakness and fainting state turn into ventricular fibrillation of the heart and its complete stop (asystole). After a couple of seconds, the blood circulation of the brain stops and the patient faints. Immediately before, symptoms such as involuntary muscle contractions, noisy breaths, pallor and a gray tint of the skin occur.
After another 2 minutes, the pupils expand to their maximum size, and visual reflexes disappear. After 3 minutes, breathing stops completely, irreparable processes occur in the brain.
Diagnostics
To prescribe effective therapy, it is necessary to establish the cause of the disease. On examination, the doctor sees the characteristic position of the patient's body, the blue tint of the lips, the bulge of the veins on the neck. Listening to the heart gives the concept of rhythm disturbance, the presence of tachycardia up to 120 or more beats per minute. A cardiologist measures blood pressure, which indicates hypertension. Also, the doctor listens to the lungs for the presence of altered breathing, palpates the liver.
The electrocardiogram is made and deciphered by the team immediately in the ambulance. Upon arrival of the patient at the medical facility, the diagnosis is carried out according to the following algorithm:
- Ultrasound examination. With its help, not only a diagnosis is established, but also possible compensatory circulatory systems are determined.
- According to blood tests, signs of hepatic and renal ischemia are revealed, it is determined how pronounced oxygen starvation is, products of destruction of the heart muscle are observed.
- Thanks to radiography, you can see the degree of expansion of the cardiac boundaries, how much more fluid is in the tissues of the lung.
Based on all these results, it is possible to determine the most effective way of treatment: medical or surgical. Diagnosis of the disease is not particularly difficult, but emergency care is already much more difficult to provide to the patient. In order to avoid irreversible consequences, at the slightest symptoms of the disease, an immediate appeal to a cardiologist is necessary. The doctor prescribes therapy for hypertension and ischemia, control of blood pressure, sugar and cholesterol levels. Be sure to regularly undergo an ECG study for children with predisposing heredity. Their treatment should begin with timely preventive measures.
Treatment
 First aid before the arrival of doctors includes the following actions:
First aid before the arrival of doctors includes the following actions:
- It is necessary to give the victim a semi-sitting posture. In this case, the limbs, both upper and lower, should be in a lowered state. This will ensure the outflow of blood from the heart and make breathing easier.
- If the attack happened in the room, it is necessary to open everything that is possible so that the air freely enters the room. Remove clothing that interferes with breathing, unbutton.
- Controlling the pressure, you can offer a person a Nitroglycerin tablet under the tongue. Repeat this action is allowed up to three times with a break of 5-10 minutes.
- Such actions can prevent pulmonary edema. On the arms (in the area of the shoulders) and legs (the area of the hips), tourniquets are applied, moderately squeezing. Give the patient a breath of alcohol, in which a piece of cotton wool must first be moistened, it is brought to the nostrils.
- If there is no pulse and breathing is gone, you should massage the heart muscle and artificial ventilation of the lungs.
After the stage of carrying out urgent pre-hospital measures, the patient is urgently taken to the hospital. Treatment continues in the hospital. If, after first aid is provided, the patient returns to full health, then he may refuse treatment within the walls of the hospital. But after 6 hours, the ambulance team must leave to check his condition of the patient or give the call to the local polyclinic.
If an attack occurred in a person with a chronic form of the disease, then this is a reason to review and adjust the previously prescribed therapy.
The main activities carried out in the hospital are the use of drugs:
| Means | Action |
|---|---|
| Positive inotropic agents (Norepinephrine, Dopamine, Dobutamine, Phosphodiesterase III inhibitors, Digoxin) | They are used on a temporary basis, as they increase the need for oxygen in the heart muscle. Increase myocardial contractility. |
| Vasodilators (Nitroglycerin, Sodium Nitroprusside and others) | Reduce the load on the heart, dilate the veins and arterioles, reduce pulmonary pressure, reduce peripheral vascular resistance and blood pressure. Unacceptable for use under reduced pressure. |
| Morphine | It is a narcotic. It has analgesic and sedative effects. Stops pulmonary edema, eliminates pain behind the sternum, which does not disappear after taking nitroglycerin. It has a number of side effects (nausea and vomiting, an attack of bradycardia, worsening of breathing, arterial hypotension). |
| Beta blockers | Reception is unacceptable for violations of myocardial contractility. Stops swelling of the lungs. |
Urgent help from surgeons can save the situation in some cases. Actual surgical intervention will be in diseases of the cardiovascular system, which led to an acute attack of myocardial insufficiency: dissection and rupture of an aortic aneurysm, valvular defects, acute aortic regurgitation, chronic cardiomyopathy in the stage of decompensation and other pathologies.
Surgical treatment may include the following operations:
- myocardial revascularization;
- prosthetics, reconstruction of valve leaflets;
- correction of other congenital heart defects;
- connection to the system of temporary maintenance of blood circulation.
- Asparagus officinalis can improve metabolism in the heart and provide its nutrition. All elements of the plant are involved in the treatment. They must be crushed, measured out 3 teaspoons of raw materials, poured with boiling water and insisted for 2 hours in an airtight container. You can use a thermos for this purpose. It is necessary to drink the infusion every two hours in the amount of 1 tablespoon.
- Lovage root helps well against edema. It makes a good diuretic. They make such a tincture for alcohol: for 250-300 g of alcohol, take 100 g of a dry plant. Put a tightly closed container in a dark place for 14 days. Then drink a tablespoon before meals three times a day.
- Natural cardiac glycosides are found in lily of the valley. They are necessary to improve the performance of the heart. But it is dangerous to use such substances without a doctor's prescription. The infusion is prepared as follows: take a glass of boiling water on a teaspoon of freshly picked flowers. Brew for half an hour, strain and take a tablespoon three times a day.
- Good sedatives will be infusions and decoctions prepared on the basis of motherwort, mint, valerian, lemon balm, fennel, hawthorn.
Any manifestations of the disease should serve as an incentive to call an ambulance, examine and further treat the causes of an attack. The prognosis for acute heart failure depends on how quickly help is provided, how severe myocardial disorders are and on the condition for the development of an emergency. According to statistics, more than half of all cases end in death. This is especially true for the elderly and children. Other, no less dangerous, consequences in acute heart failure occur in the form of such pathologies: bronchopneumonia, renal or hepatic failure, pulmonary edema, embolism, stroke. The diagnosis of "acute heart failure" is a reason to be extremely careful about your health.
Article publication date: 12/18/2016
Article last updated: 12/18/2018
From this article you will learn: what is acute heart failure, what are its types, the most common causes. Symptoms, special treatment, how to help the patient at home.
Acute heart failure is a sudden and life-threatening pathological condition in which the heart is completely unable to pump blood. In contrast to chronic heart failure, which can proceed “sluggishly” and for several years, in the acute form, the symptoms appear abruptly and last for several minutes or hours.
This syndrome is the most severe complication of all heart diseases, carries an immediate threat to life and in 45–60% ends in the death of patients. It is classified as an emergency requiring emergency medical attention.
The condition of patients with any form of acute heart failure is critical - they are forced to be in a lying or sitting position, suffocate at rest. Therefore, treatment should be conservative (medication, correct body position, oxygen) in the mode of urgent measures aimed at saving lives.
The treatment process is carried out by doctors of two specialties: a cardiologist or a therapist with the obligatory participation of a resuscitator. Patients with acute heart failure are hospitalized in the intensive care unit.
The essence of pathology, its types
The ventricles are responsible for pumping blood around the body. There are two in total:
- The left one is more powerful, takes blood from the lungs, provides movement through the vessels of the whole body, supplying them with oxygen-rich blood (systemic circulation - limbs, internal organs, brain).
- The right one takes blood from the veins of the whole body, pumps it in a small circle (only through the vessels of the lungs), where oxygen is absorbed.
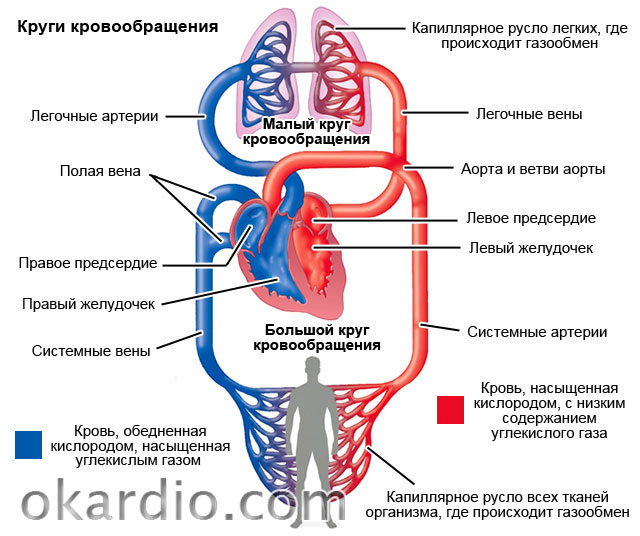
If any of the ventricles of the heart suddenly fails to perform its pumping function, a severe circulatory disorder occurs in the corresponding vascular circle.
Depending on which ventricle is more affected, acute heart failure can be:
- Left ventricular - there is stagnation of blood in the lungs, and all other tissues experience oxygen starvation.
- Right ventricular - stagnation of blood in all tissues, insufficient blood flow to the lungs.
- Combined or biventricular - when both ventricles are affected.
In 70–75%, the function of the left ventricle is primarily impaired, in 25–30% of the right. Combined biventricular insufficiency of the heart can be if the treatment does not work. Its occurrence indicates the complete insolvency of the myocardium and in 90-95% ends in death.
Causes
Common causes of acute left ventricular heart failure
Two groups of reasons:
- Cardiac (cardiac) - heart disease, leading to a critical violation of the structure and function of the myocardium (heart muscle) - in 93-97% of cases.
- Extracardiac - severe diseases and damage to internal organs, which lead to secondary damage to the myocardium.
| 1. Cardiac causes | 2. Non-cardiac causes |
|---|---|
| Myocardial infarction (necrosis) | Hepatic and renal insufficiency |
| Myocarditis (inflammation of the myocardium) | Alcohol abuse |
| Acute cardiac arrhythmias (fibrillation, fibrillation, extrasystole) | Poisoning with toxic substances and medicines |
| severe hypertensive crisis | Malignant tumors with metastases |
| Congenital and acquired malformations of the heart and valvular apparatus | Severe or long-term anemia |
| Progression and complete decompensation of chronic heart failure | Diseases of the thyroid gland (thyrotoxicosis, hypothyroidism), adrenal glands (insufficiency, pheochromocytoma) |
| Cardiomyopathy of any kind | Sepsis and severe infections |
| Heart injury (wounds, concussion) | Volumetric stroke of the brain |
| Postpartum cardiopathy | Severe operations, injuries, burns |
 Cardiomyopathy is one of the causes of acute left ventricular heart failure.
Cardiomyopathy is one of the causes of acute left ventricular heart failure. Causes of right ventricular heart failure
Acute heart failure of the right ventricle differs from left ventricular failure in terms of causes and mechanisms of development. Most often these can be:
- (large branches) - blockage of the vessels of the lungs by blood clots;
- massive infarction of the right ventricle or interventricular septum;
- overflow (tamponade) of the pericardium with blood as a result of an injury;
- chest trauma, accompanied by damage to the lungs, accumulation of air and blood in the pleural cavities (valvular pneumothorax, hemothorax);
- pleurisy and pericarditis (inflammation of the pericardium and pleura, accompanied by the accumulation of a large amount of fluid);
- massive unilateral or bilateral pneumonia (pneumonia);
- severe course of bronchial asthma and status asthmaticus.
Theoretically, the common cause of acute failure of both the right and left ventricles of the heart can be any of the cardiac and non-cardiac factors. But in practice, such a pattern is observed that all heart diseases and other pathological conditions occur with a predominant lesion of the myocardium of the left ventricle. Therefore, they are complicated by acute left ventricular heart failure.
The right ventricle becomes insolvent mainly (in 90–95%) due to acute pathology of the lung tissue. As a result of its rapid restructuring, the myocardium cannot overcome the increased resistance exerted by the pulmonary vessels at the time of blood ejection.
Degrees of heart failure
The division of acute heart failure into severity is determined by the severity of symptoms. The more severe the manifestations, the higher the degree.
Symptoms
In 80-90% of cases, the clinical picture of acute heart failure always develops very quickly and suddenly (within minutes) and can last up to several hours. In the remaining 10–20% of cases, manifestations increase gradually. Symptoms depend on:
- causes of occurrence;
- degree of circulatory disorders;
- localization of the affected ventricle (right or left).

Left ventricular failure
The main symptoms and manifestations of acute left ventricular heart failure, taking into account significant factors, are described in the table:
| Severity | Symptoms that characterize the severity |
|---|---|
| cardiac asthma | Sudden shortness of breath, choking, feeling short of breath |
| Anxiety, anxiety, feeling of fear | |
| Rapid breathing (more than 22–25/minute), shallow | |
| Forced sitting position, inability to lie down | |
| Blueness of the fingers, toes, tip of the nose, and ears | |
| Pale skin and face, clammy cold sweat | |
| Decreased blood pressure (up to 100/60 mmHg) | |
| Pulmonary edema | Severe shortness of breath and choking, rapid breathing (more than 25/minute) |
| Rattling wheezing that can be heard at a distance | |
| Dry cough with occasional frothy sputum | |
| Complete inability to breathe while lying down | |
| Weak frequent pulse (more than 110 beats), deafness of heart tones | |
| Multiple moist rales on auscultation of the lungs | |
| Other symptoms characteristic of cardiac asthma | |
| Cardiogenic shock | Confusion (lethargy) or lack of |
| Decreased blood pressure less than 90/60 mm Hg. | |
| Severe pallor of the skin with a marbled bluish tint | |
| Lack of urine | |
| All other symptoms of pulmonary edema and cardiac asthma |
 Symptoms of left ventricular failure
Symptoms of left ventricular failure Development of symptoms:
- Heart failure of the left ventricular type begins with symptoms of stagnation of blood in the small circle and lung damage (shortness of breath).
- As the pressure in the vessels increases, the blood begins to saturate the lung tissue, as a result of which it swells and breathing becomes impossible at all.
- If these changes are not eliminated, they lead to depletion of the blood with oxygen, which further aggravates the condition of the heart.
- The last stage is the disruption of the brain and all internal organs, the cessation of contractile activity of the myocardium, a critical decrease in blood pressure. All this leads to death.
Right ventricular failure
If the right ventricle of the heart becomes insolvent, symptoms of blood stagnation occur in the largest veins of the body - the superior and inferior vena cava. This condition is called acute cor pulmonale. Its manifestations:

Mandatory diagnostic methods
All patients with signs of acute heart failure require additional diagnostics:
- ECG (electrocardiography);
- chest x-ray;
- pulse oximetry (measurement of oxygen tension in the blood);
- general blood analysis;
- ECHO-cardiography (ultrasound of the heart);
- other methods to clarify the cause of acute heart failure: a blood test for troponins, a coagulogram, a biochemical study.
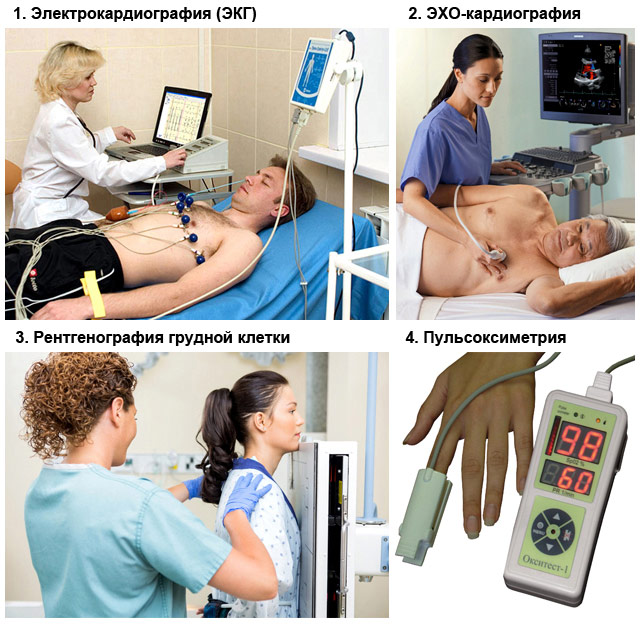 Methods for diagnosing acute heart failure
Methods for diagnosing acute heart failure Methods and stages of treatment
Since acute heart failure is an acute condition, therapeutic measures to eliminate it should be urgent. The road is literally every minute. As soon as this problem is suspected, help should be started.
First aid measures at home
- Call an ambulance by calling 103!
- Provide the patient with the desired body position: half-sitting, legs and arms lowered down, it is imperative that there is support under the back and head. The lowered limbs will retain blood, which will reduce the load on the heart, and the semi-sitting position of the body will reduce shortness of breath.
- Create conditions for free access of fresh air to the patient - free the chest and neck from clothes and other items, open the window, window or door in the room.
- If symptoms of pulmonary edema appear, it is recommended to apply moderately compressive tourniquets to the lower and upper limbs (at the level of the shoulders and hips);
- Let the patient, together with the inhaled air, inhale the vapors of ethyl alcohol or a strong alcoholic drink (vodka). Soak a cotton pad with them and place near the nose. Alcohol is a good defoamer and prevents the progression of pulmonary edema.
- Determine the pulse, respiratory rate and pressure. If they are absent, this indicates clinical death. Start resuscitation: pressure on the lower third of the sternum (heart massage) about 100 r / min, artificial respiration. Before performing them, lay the patient on his back on a hard surface, tilt his head back, clear the oral cavity of mucus and foreign objects (prostheses, vomit, etc.).


Medical treatment
Acute heart failure can be cured only through complex drug therapy. It includes:
1. Pain relief and fear relief
For this, drugs are administered intramuscularly:
- Analgin or Ketanov in combination with Diphenhydramine;
- Narcotic analgesics - Morphine (preferably), Promedol, Omnopon (in the absence of Morphine).

2. Stimulation of cardiac activity
- Dopamine - increases the strength and frequency of heart contractions (accelerates the heart), increases blood pressure. It is administered as an intravenous dropper in high doses at low pressure, in low doses at normal or elevated pressure, in combination with pulmonary edema.
- Mezaton, Norepinephrine - mainly increase blood pressure, stimulate the myocardium with minimal effect on the frequency of contractions. The most appropriate intravenous injections or droppers for cardiogenic shock.
- (Digoxin, Strofantin) - increase the strength of heart contractions, slowing down their frequency. Do not affect blood pressure. Contraindicated in myocardial infarction.

3. Decrease in venous return of blood to the heart, unloading of the ventricles
- Nitrates - preparations Nitroglycerin, Isoket, Nitro-mic. It can be given to the patient either in the form of tablets under the tongue every 5-10 minutes or administered intravenously (put a dropper) under pressure control.
- Beta blockers (drugs Metoprolol, Anaprilin) - a tablet under the tongue.
- Diuretics (drugs Furosemide, Lasix, Trifas). It is best to administer intravenously in high doses.

4. Other activities and drugs
- Continuous inhalations of humidified oxygen with ethanol vapors.
- Intravenous administration of glucocorticoid hormones (drugs Prednisolone, Dexamethasone, Hydrocortisone).
- Drugs that dilate the bronchi - Eufillin.
- Specific medicines for the treatment of major diseases (pulmonary embolism, myocardial infarction, arrhythmia) - anticoagulants (Heparin), (Amiodarone, Aritmil, Verapamil, Lidocaine).

If the cause of heart failure is caused by injuries, wounds to the heart and chest, pathological accumulation of fluid in the pleura or pericardium against the background of inflammation, patients need urgent surgical treatment - puncture or drainage into the appropriate cavity to pump out effusion (blood, pus).
Outcome and forecast
Acute heart failure is characterized by disappointing general statistics - about 50-60% of patients die. The outcome depends on the cause, severity and timeliness of treatment of this complication. With proper treatment, the prognosis is as follows:
- If the cause or massive pulmonary embolism - mortality exceeds 90%.
- Initial symptoms in 90% are successfully resolved against the background of drug treatment.
- The success of the treatment of manifestations of acute heart failure in the form of - 60-70%.
- The stage of pulmonary edema is resolved in 50%.
- Cardiogenic shock in 80-90% ends in death.
Despite the sad statistics, in no case do not give up. Life is one and you have to fight for it. Moreover, efforts are rewarded!
Every year, diseases of the cardiovascular system lead to the death of more than 17 million people worldwide. Only in 10% of cases such pathologies are congenital. The vast majority of painful conditions occur against the background of stress and the wrong way of life of a modern person. In the article we will understand what acute heart failure is.
Symptoms before death and complications caused by pathology, methods of diagnosis and treatment of the disease, types and forms of the disease - information on all these issues will be reflected in the materials of our review. In addition, the article mentions rules of conduct that can be useful to any of us. The ability to act correctly in a critical situation in most cases ensures the preservation of human life. In accordance with this, everyone should know what first aid is for acute heart failure.
The concept of heart failure
Heart failure (HF) is a pathology in which the heart stops supplying the tissues of the body with the necessary amount of blood. It is a consequence of the impaired ability of the heart muscle (myocardium) to contract. HF leads, as a rule, to severe clinical manifestations, including heart attack, cardiogenic shock.
Both men and women are susceptible to the disease, but the latter suffer from this disease more often. Mortality from pathology is quite high. Danger to human life is any of the manifestations caused by a disease such as acute heart failure. Symptoms before death, called sudden death in medicine, are very diverse. They depend on what form of the disease occurs. According to the nature of the origin of heart failure, there are:
- Myocardial heart failure is a pathology that is the result of direct damage to the heart muscle due to a violation of energy metabolism. This type of heart failure results in impaired contraction and relaxation of the heart.
- Overload heart failure is a pathology that develops as a result of a large load on the heart. This type in some cases develops against the background of heart defects.
- Combined heart failure is a form of pathology that combines the causes of the two above.
Classes of heart failure
To date, there are various criteria by which the disease is divided into types or forms. Medicine knows several classification systems (Russian, European, American), but the most popular is the system proposed by US cardiologists. In accordance with this technique, four classes of the disease are distinguished:
- Class 1, in which the patient has shortness of breath with active movement, for example, climbing stairs to a level above the third floor.
- Class 2, in which shortness of breath appears even with a slight load - when climbing to the first or second floor. At the same time, there is a decrease in physical activity of a person.
- Grade 3, in which heart failure is noticeable with minor exertion, for example, when walking, but at rest, the symptoms of the pathology disappear.
- Class 4, in which the symptoms of the disease appear even at rest, and slight physical activity leads to serious disturbances in the work of the heart and the entire vascular system as a whole.
CH classification
Pathology can be classified according to several criteria. Depending on the clinical picture of the course of the disease, acute and chronic heart failure is known to medicine.
Acute heart failure (AHF) is a disorder in which the symptoms of the pathology appear quickly (within a few hours). As a rule, against the background of other diseases of the vascular system, acute heart failure occurs.
Heart attack, myocarditis and other diseases can become a trigger for painful conditions, because with these pathologies, heart muscle cells die due to local circulatory disorders. AHF can also result from rupture of the walls of the left ventricle, acute valve insufficiency (aortic and mitral). In some cases, the pathology develops without previous disorders.

AHF is a rather insidious disease, because it can cause painful conditions in other body systems. Complications of acute heart failure often affect not only the heart, but also the respiratory organs, causing pulmonary edema, cardiac asthma, and cardiogenic shock.
Chronic heart failure is a disorder in which the pathology develops gradually over weeks, months, or even years. Occurs against the background of heart disease, arterial hypertension or prolonged anemia.
Types of AHF according to the type of hemodynamics
Depending on the type of hemodynamics characteristic of the location of the pathology, there are the following forms of acute heart failure:
- AHF with congestive hemodynamics.
- AHF with hypokinetic type of hemodynamics.
Hemodynamics is the flow of blood through the vessels, which is due to the excellent pressure in various areas of the circulatory system. It is known that blood moves from an area of higher pressure to an area of lower pressure.
The pressure directly depends on the viscosity of the blood, as well as on the resistance of the vessel walls to the blood flow. AHF with congestive hemodynamics may involve the right or the heart. Accordingly, there are:
- Acute right ventricular failure, in which venous congestion is observed in a large circle of blood flow, i.e., affects almost all organs and tissues.
- Acute left ventricular failure, in which venous stasis occurs in a small circle of blood flow. Pathology causes a violation of gas exchange in the lungs and leads to the development of pulmonary edema or cardiac asthma. Thus, against the background of such disorders, acute pulmonary heart failure occurs.
AHF with hypokinetic type of hemodynamics
Acute heart failure with a hypokinetic type of hemodynamics is a pathology caused by cardiogenic shock - a sharp decrease in the ability of the myocardium to contract, which leads to disruption of the blood supply to all tissues of the body.
Distinguish:
- Arrhythmic shock, which is the result of an abnormal heart rhythm.
- Reflex shock is a reaction to pain.
- True cardiogenic shock is a pathological condition that occurs when the tissue of the left ventricle is damaged, and the affected area is at least 50%. As a rule, persons over 60 years of age are more susceptible to the violation; people who have had a second heart attack; patients with arterial hypertension and diabetes mellitus.
It is important to note that cardiogenic shock is characterized by pain, a sharp decrease in blood pressure to minimal values (down to 0), a threadlike pulse, and pallor of the skin. Pathology can later turn into pulmonary edema or end in renal failure.
Factors contributing to the occurrence of AHF
The development of acute heart failure in a patient may be preceded by pre-existing systems. These states include:
- heart disease caused by damage to the heart muscle, leading to a sharp decrease in the ability of the myocardium to contract;
- chronic heart failure, in which the normal blood supply to organs and tissues is disturbed;
- damage to the integrity of the heart valves and chambers;
- accumulation of fluid in the pericardial sac, which leads to a violation of the correct rhythm of heart contractions due to the pressure exerted on the cavity of the heart (this pathology is called cardiac tamponade);
- thickening of the walls of the heart - myocardial hypertrophy;
- hypertensive crisis - a pronounced deviation of blood pressure from the norm.
non-cardiac reasons
In addition to heart problems, pathologies associated with increased pressure in the pulmonary circulation of blood can be involved in the occurrence of painful conditions. Diseases leading to the diagnosis of "acute heart failure":
- stroke - a violation of the blood circulation of the brain, which provokes damage to its tissues and a general disorder of brain functions;

- thromboembolism of the pulmonary artery (this disease occurs due to blockage of the pulmonary artery, as well as its processes with blood clots (thrombi), most often blood clots occur in the large veins of the pelvis and lower extremities);
- lung diseases - inflammation of the bronchi (bronchitis), inflammation of the lung tissue (pneumonia);
- violation of the rhythm of heart contractions (acceleration or deceleration) - tachyarrhythmia, bradyarrhythmia;
- infections caused by various pathogens.
There are also factors that lead to the development of HF, but are not a manifestation of diseases of any body systems. These include:
- surgical intervention;
- trauma and brain damage;
- toxic attacks on the heart muscle - alcohol, aggressive drug exposure;
- the use of which leads to certain consequences;
- electrical injury - the impact on the body of an electric current;
- psycho-emotional or physical stress.
Diagnosis of acute heart failure
Diagnosis of heart failure is aimed primarily at establishing the causes that led to the development of pathology. Before conducting laboratory tests and manipulations using medical equipment, the doctor determines through a conversation with the patient the presence or absence in his life of certain factors that contribute to the development of such a pathology as acute heart failure. Symptoms before death (sudden), occurring within 24 hours, may be mildly manifested, and the task of the specialist is not to waste time, but, taking into account all the patient's complaints, establish the correct diagnosis as soon as possible.
The main research methods used in the diagnosis of AHF include:
- electrocardiogram;
- echocardiogram;

- chest x-ray;
- general and advanced blood tests;
- sometimes, for the diagnosis of AHF, a cardiovisor is used - a device whose principle of operation does not differ from an electrocardiograph.
Diagnostic criteria
The main and most pronounced symptom of an acute course of heart failure can be called sinus tachycardia - a form of supraventricular tachyarrhythmia, which is characterized by an accelerated sinus rhythm - the heart rate in an adult exceeds 100 per minute. A graphical representation of the activity of the heart illustrates the extended boundaries of the organ to the left or right. In addition, a third tone appears at the apex or above the xiphoid process.
Acute congestion is manifested by several signs:
- the neck and liver veins swell and swell;
- high venous pressure;

- enlargement of the liver, yellowness of the integument;
- swelling of the limbs;
- cyanosis of the fingers, face (ears, chin, tip of the nose);
- the patient experiences severe pain in the hypochondrium on the right;
- The ECG of the heart captures a sharp overload of the right ventricle and atrium, which is expressed by high pointed teeth.
Signs of right ventricular failure are clearly identified by X-ray examination and electrocardiogram. The final stage of this type of cardiac pathology leads to the exhaustion of the body, a decrease in the level of protein in the blood and a violation of the salt balance in the human body.
Signs of left ventricular failure and cardiogenic shock
In turn, the presence of acute left ventricular failure with congestive hemodynamics is evidenced by a number of the following signs:

There are a number of characteristic symptoms of cardiogenic shock, namely:
- The patient's blood pressure drops to values of 90-80 mm Hg. Art. and even less. If a person suffers from arterial hypertension, then a sign of shock will be a decrease in the rate by 30 mm Hg. Art. from the daily individual level.
- Decrease in pulse pressure - less than 25-20 mm Hg. Art.
- Suspicion of cardiogenic shock should cause pallor of the skin and its coldness. These manifestations indicate a violation of blood microcirculation in the tissues of the body.
With a person who has the above manifestations of pathology, a number of measures should be taken before the arrival of specialists. First aid for acute heart failure (stroke, heart attack, etc.) should be aimed at:
- organize access to fresh air;
- ensure the horizontal position of the patient (unless he has signs of left ventricular failure);
- perform analgesic actions.
Treatment of acute heart failure
Treatment of heart failure is a complex therapy aimed primarily at:
- eliminate overload of the heart muscle - this measure is achieved by the use of drugs that reduce blood pressure and heart rate;
- stop the symptoms of pathology (therapeutic measures will depend on the manifestations of painful manifestations).
If AHF has developed as a result of myocardial infarction, it is necessary to restore the flow of the coronary artery as soon as possible. As a rule, a heart attack causes thrombosis of an artery that feeds the heart. The elimination of the thrombus helps to completely restore the patency of the blood vessel and stabilize the patient's condition.
The most popular technique in this case is thrombolysis, but the procedure should be carried out as soon as possible from the onset of a heart attack, while the clot is still “fresh”. First aid for acute heart failure involves the use of drugs (thrombolytics), the action of which is aimed at dissolving blood clots. Medicines are administered intravenously, the rate of their entry into the body is strictly regulated.
Treatment of acute failure (right ventricular) with congestive hemodynamics involves the elimination of the causes that caused it - status asthmaticus, blood clots in the pulmonary artery, etc. facilities. In conjunction with the above measures, oxygen is inhaled through a catheter.
It is eliminated by narcotic analgesics, for example, "Morphine", which reduces the work of the respiratory muscles and reduces the load on the heart.
Elimination of symptoms of left ventricular failure
Stagnation of blood in the pulmonary circulation often leads to serious consequences, such as pulmonary edema. With such violations, patients are prescribed the introduction of "Nitroglycerin" intravenously.
If acute with congestive hemodynamics is combined with cardiogenic shock, the administration of "Dobutamine" or "Norepinephrine" intravenously is prescribed. It is not uncommon for these drugs to be combined in combination.
Foaming is stopped with the help of means that ensure the destruction of the foam.
If hemodynamics is stabilized, but signs of pulmonary edema persist, the patient is prescribed glucocorticoids. In this case, first aid for acute heart failure will help reduce membrane permeability.
Therapy for cardiogenic shock begins with an increase in cardiac output, in the absence of manifestations of congestive heart failure, it includes the introduction of plasma substitutes. This procedure is performed only under the control of heart rate, blood pressure and respiration. If there was a large loss of fluid before the onset of an acute pathology of the heart, a solution of sodium chloride is used.
The elimination of the symptoms of pathology, of course, is primarily associated with the use of medications, however, if the measures taken do not lead to the desired effect, you can use the right way - to perform hemodynamic unloading by applying tourniquets to the veins of the limbs.
In cases where conservative medicine is powerless, resort to surgical treatment. In this way, problems associated with blockage of arteries, replacement of heart valves are eliminated. Installing a pacemaker or defibrillator helps stabilize the heart rate.
Prevention
The best way to prevent the development of pathology is to follow simple rules, namely, to lead a healthy lifestyle, quit smoking and stop drinking excessive alcohol, and periodically monitor existing chronic diseases. However, in cases where the disease nevertheless made itself felt, a certain regimen should be followed in everyday life.

Patients with acute heart failure should closely monitor their weight. Extra pounds provoke an increase in blood sugar and the formation of cholesterol plaques on the vessels, and this causes high blood pressure. An important condition for maintaining a normal physical condition is the observance of a special diet in nutrition. It is necessary to strictly regulate the intake of salt into the body, the excess of which has a bad effect on health - it causes fluid retention, edema is formed, and the load on the heart increases.
It is useful to perform physical exercises, to give a load to the muscles and joints, but playing sports should not cause overload of the body. A set of exercises must be agreed with the doctor. It is important to be in the fresh air often, get enough sleep, avoid stress and mental stress.
Summarizing all of the above, it can be noted that acute heart failure is a pathology that often leads to death. The disease, as a rule, develops against the background of other painful conditions of the cardiovascular system and leads to various complications, including stroke, cardiogenic shock, pulmonary edema, etc.
There are signs by which acute heart failure is diagnosed. Symptoms may be subtle before death, so an important task for specialists is to take into account all complaints of the patient and conduct immediate screening.