Bedsores begin, what to do. Risk factors for developing pressure ulcers
Bedsores– these are areas of tissue necrosis due to impaired blood circulation in them. As a rule, bedsores form when a part of the body comes into contact with a hard surface for a long time. Sooner or later, most people with limited mobility develop bedsores, but patients who are overweight, diabetic, or severely malnourished are most susceptible to them.
According to statistics, bedsores develop in 80 percent of patients who are in a supine position. Most often, pressure sores form on the heels and buttocks. The prevalence of this type of tissue damage varies from country to country. In studies conducted in South Korea, for example, pressure ulcers were diagnosed in 47.4 percent of patients in home care and 21.7 percent of patients in intensive care units. In Canada, the prevalence of pressure ulcers is 26 percent. According to British scientists, bedsores occur in 15–20 percent of patients in health care institutions. In the United States, approximately 17 percent of all hospitalized patients are at risk of developing tissue death or already have pressure ulcers. According to the testimony of American scientists, 60 thousand people die every year in their country from complications that develop against the background of pressure ulcers. In the European Union, the prevalence of bedsores in particularly severe forms reaches 150 thousand cases per year.
The search for drugs for local treatment of wounds that would combine high efficiency against wound microflora with the ability to prevent the colonization of wounds by hospital microflora and, at the same time, stimulate wound healing remains an urgent task in surgery. Pectinar surgical napkins can be recommended as an effective drug in the treatment of bedsores.
It works simultaneously in five directions:
1. BACTERICIDAL ACTION
Pronounced selective bactericidal effect on pyogenic microflora (Pseudomonas aeruginosa, Staphylococcus aureus, streptococci, Klebsiella, Proteus, etc.), while beneficial microflora is not sensitive to it. The bactericidal activity of PECTINAR is comparable to that of antibiotics.
2. ANTI-INFLAMMATORY ACTION
In all cases of using PECTINAR, the local use of antibiotics and other antibacterial agents is eliminated, which significantly saves money on expensive drugs and eliminates the occurrence of side effects.
3. PROTECTIVE ACTION
When applied, it forms a protective film on the surface of the wound, relief covering the affected tissue of any configuration, thereby preventing the penetration of pathogenic microflora into the wound, including protecting the wound from colonization of hospital microflora.
4. REGENERATING ACTION
Retains environmental moisture in the wound, which promotes recovery processes and accelerates healing.
5. SORBENT ACTION
Sorbs bactericidal toxins and tissue breakdown products, which promotes the activation of immune processes.
Compound:
stabilized 3% pectin solution (natural polymer of D-galacturonic acid), sterile medical gauze wipes 14x16 cm, two-layer. Sold in pharmacies. The problems of tissue necrosis have been known to mankind for a long time. The first literary mentions of bedsores go back thousands of years and belong to Hippocrates. The French surgeon Ambroise Paré identified the elimination of pressure as the main condition for successful treatment of bedsores. Another French scientist Brown-Séquard in 1852 published his opinion that, in addition to compression, the occurrence of pressure wounds is influenced by high humidity skin. In the mid-20th century, disorders of the autonomic nervous system also began to be considered as causes of tissue necrosis. Before the onset of the 21st century, bedsores were treated mainly surgical method. The ulcers were closed with transplanted skin flaps, excised, and in some cases, bone tissue was removed under the bedsore. Since the end of the 20th century, in the fight against pressure ulcers, world medicine began to pay great attention to the prevention of pressure ulcers. Thus, between 1990 and 2008, the number of publications on topics such as practical guidelines for caring for bedridden patients, the development of risk assessment scales and prevention programs increased by 960 percent.
The average cost of treating pressure ulcers in hospitals in the United States is approximately $11 billion per year. The annual costs of the UK's National Health Service range from £1.4 billion to £2.1 billion, representing around 4 percent of the organisation's total costs. The cost of monthly out-of-hospital treatment for a patient with bedsores in Canada is 9 thousand US dollars.
Treatment and prevention of pressure ulcers has changed over time. So, in ancient times, to alleviate the condition of the patient, a copper basin filled with water was placed under his bed. Another remedy with a more understandable mechanism of action was a bull bladder, which was filled halfway with air and placed under the body of a sick person. This device was a prototype of a modern device for preventing the development or complications of bedsores. One of the effective developments of today is the Mepilex Border bandage, developed by specialists from Molnlycke Health Care. Currently, about 15 studies have been published confirming the high results of using this product.
An interesting study was conducted by American scientists from Medical Nutrition USA. The result of their work was the proven fact that the diet and quality of nutrition greatly influence the speed of healing and restoration of affected tissues during bedsores.
A team of engineers from the University of California has developed a “smart” bandage that provides the ability to prevent bedsores. The device appears to be in the form of a belt containing electrodes. The device unit delivers weak electrical impulses and if the cellular tissues are viable, they do not conduct current. If a cell begins to die, its conductivity of electricity is maximum. By analyzing this characteristic of cells, the device identifies affected areas that have not yet turned into bedsores, which makes it possible to take appropriate measures in a timely manner. The bandage was tested on rodents, and at the moment the developers are going to recruit volunteers to continue the study.
Skin structure, blood supply and innervation
 The skin plays the role of the largest organ of the human body, making up 15–17 percent of the total body weight. The skin has a rather complex structure, divided into layers and sublayers.
The skin plays the role of the largest organ of the human body, making up 15–17 percent of the total body weight. The skin has a rather complex structure, divided into layers and sublayers. The main layers of the skin are:
- epidermal layer;
- basement membrane;
- dermal layer;
- hypodermal layer.
Main characteristics of skin layers
| Skin layer | Layer structure | Thickness | Main functions |
| Epidermal layer | 5 sublayers. | 0.05 – 0.15 millimeters ( 0.8 – 1.5 millimeters in the skin on the elbows, knees, palms and feet). |
|
| basement membrane | 2 thin plates. | up to 90 nanometers ( 0.00009 millimeters). |
|
| Dermal layer | 2 sublayers. | from 0.5 millimeters to 4 - 5 millimeters. |
|
| Hypodermal layer | one layer without clear boundaries. | from 2 – 3 millimeters to 10 – 12 or more. |
|
Epidermal layer ( epidermis)
The epidermal layer is the outer visible layer of the skin. It consists of a large number of epithelial cells ( structural cells of the epidermal layer) of varying sizes and degrees of maturity, grouped into five layers. Skin epithelial cells have the form of flat cells. In the superficial layers, the epidermis consists of “obsolete” and keratinized ( dead) epithelial cells. Thus, the entire layer of epithelial cells of the dermis is called stratified squamous epithelium.Sublayers of the epidermis
| Sublayer | Structure | a brief description of |
| Horny | 3 – 5 rows of “dead” cells. |
|
| Brilliant | 2 – 4 rows of cells that do not contain a nucleus. |
|
| Grainy | 1 – 5 rows of small cells containing many granules. |
|
| Spiky | 3 – 8 rows of cells with spine-shaped outgrowths. |
|
| Basal (deepest layer) | one row of large cells. |
|
Cells of the three lower layers ( basal, spinous and granular) are living cells that possess a cell and cytoplasm. Epithelial cells of the stratum lucidum and stratum corneum, lacking a nucleus, are dead cells. All life processes in them have ceased.
The epidermal layer is devoid of any blood vessels and lymphatic vessels. Nutrients and water enter through the basement membrane from the dermal layer.
Change of skin epidermis
The skin is the only organ ( except for the liver), which has the property of regeneration. It is constantly updated and is restored quite quickly in case of various damages.
The process of changing the epidermis occurs smoothly in several stages:
- formation of new cells;
- cell migration from layer to layer;
- reduction of the nucleus and flattening of the cell;
- loss of all organelles ( intracellular components) and water;
- filling the cell with keratin and keratinization;
- loss of intercellular contacts and exfoliation of dead cells.
The full cycle from the birth of a new cell to its exfoliation from the skin is 27 – 27 days. Thus, every month human skin is completely renewed.
Dermal layer ( dermis)
The dermal layer consists of a number of cells and connective tissue fibers that form two sublayers - papillary and reticular. Both layers have their own structural features and perform different functions.Characteristics of the sublayers of the dermis
| Sublayer | Main function | Main cast | Additional skin elements |
| Papillary | Nutrition of the epidermal layer. |
|
|
| Reticular
(Reticulate) | Ensuring skin strength and elasticity. |
|
|
Papillary sublayer of the dermis
The papillary sublayer is located under the basement membrane, to which it is closely adjacent. Many small capillaries ( arterioles and venules) form vascular glomeruli in this layer. Thin bundles of collagen and elastin fibers surround these glomeruli, forming the papillae. The papillae are wedged into the epidermal layer, providing a large extent of contact surface between the layers.
Reticular sublayer of the dermis
The reticular layer is the thickest sublayer of the dermis. Thick collagen and elastin fibers intertwine to create the underlying, strong framework of the skin. Collagen fibers give the skin strength, and elastin fibers provide its elasticity and firmness.
The entire space between the network of intertwined collagen and elastin fibers is occupied by hyaluronic acid. It forms many cells in which it holds water. Once saturated with moisture, hyaluronic acid turns into a gel. This gel keeps the skin elastic, creating a soft frame.
Fibroblasts are located in the intercellular substance near the fibers ( connective tissue cells), which continuously synthesize and destroy collagen, elastin and hyaluronic acid in a vicious circle.
Hypodermal layer ( hypodermis)
The hypodermal layer is the deepest layer of the skin. Its thickness varies different areas body and varies from person to person. Particularly thick hypodermis is observed in the areas of the thigh, buttock and abdomen.The hypodermal layer does not have a clear boundary separating it from the dermal layer, since the fibers of the connective tissue of the dermis thicken and pass into the hypodermis. Thick collagen and elastin fibers continue to intersect and form a network.
The main cellular element of the hypodermal layer is the adipocyte ( fat cell). Therefore, this layer is also called the subcutaneous fat layer. Adipocytes fill all the space in the cells of the “collagen-elastin” network. Their number is constant. An increase in the thickness of adipose tissue occurs due to the accumulation of fat in cells and an increase in their size.
In the hypodermal layer between the adipocytes there are some important elements of the skin involved in its nutrition and protection.
The main elements of skin in the hypodermis are:
- nerve fibers;
- veins;
- arteries;
- network of lymphatic vessels;
- hair follicles;
- sweat glands.
Blood supply to the skin
The epidermal layer of the skin is completely devoid of blood vessels. All nutrients penetrate into this layer from the dermis by simple diffusion ( transition). The dermis, in turn, receives nutrition from a well-developed network of vessels that originate in the hypodermis or in deeper layers ( fascia and muscles).Arteries, veins and lymphatic vessels form several main plexuses in the dermis and hypodermis, which give rise to many small branches.
Vascular networks of the skin
| Vessels | Networks | Location |
| Arteries | deep dermal network | hypodermal layer, just below the dermis |
| subpapillary network | between two layers of dermis | |
| Vienna | subpapillary plexus | under the papillary dermis |
| reticular plexus | middle of the reticular layer of the dermis | |
| deep cutaneous venous network | hypodermal layer | |
| Lymphatic vessels | surface network | papillary dermis |
| deep web | reticular layer of dermis |
Arteries
Large arteries from the fascia and muscles give branches to the hypodermal layer. In the hypodermis, the arteries are closely intertwined, forming a deep skin network. Many smaller vessels depart from this network, which supply blood to the cells of the hypodermis, hair follicles and sweat glands. Some of the small vessels from the deep skin network are directed upward to the dermal layer. At the level of the dermis, they give new branches that nourish the dermis itself and the structures located in it ( sweat and sebaceous glands, hair follicles). Having reached the papillary layer, the arteries are closely intertwined into a new network - the subpapillary. Many arterioles emerge from it ( smallest branches of arteries), which connect to venules ( the smallest branches of veins). The connection of the arterial blood flow with the venous blood flow occurs in the papillae of the dermal layer.Vienna
Venules give rise to the first venous plexus, located under the papillary layer. The subpapillary venous plexus collects “used” blood and all waste products from cells of both the papillary layer and the epidermis. Next, the veins are directed to the reticular layer, where they form the second venous plexus. It becomes a blood collector for the entire dermis, hair follicles and glands. Next, venous blood enters larger veins and descends into the hypodermal layer. Here the third, largest venous network of the skin is formed - the deep cutaneous venous network. It collects venous blood from all cells and structures of the hypodermal layer. The deep venous network gives rise to larger veins located under the skin.Lymphatic vessels
Lymphatic vessels of the skin follow the trajectory blood vessels, nourishing all structures and skin cells. They form two large networks – deep and superficial. Both of them are located in the dermal layer. The superficial plexus is located at the level of the papillary layer, sending its small capillaries up into the papillae. A deep network is formed in the reticular layer of the dermis. Large lymphatic vessels depart from it to all elements of the dermis and hypodermis.The main feature of all skin vessels is their ability to quickly narrow and expand. This occurs reflexively when nerve receptors in the skin are irritated.
The main external stimuli can be:
- low and high temperatures;
- chemical substances;
- mechanical stimuli ( friction, prolonged pressure, impacts).
Innervation of the skin
Innervation of the skin occurs due to a wide network of nerve fibers and nerve endings that follow the trajectory of the vessels.Cutaneous branches arise from the spinal and cranial nerves. In the hypodermal layer, the cutaneous branches form a large nerve plexus of the skin. Thinner nerve branches are directed into the dermis, forming two nerve plexuses - deep and superficial. The deep plexus is located at the level of the reticular layer of the dermis. The superficial plexus is formed under the papillae of the dermal layer. Some of the fibers are directed into the papillary layer and into the epidermis, ending in sensory receptors.
From all the nerve plexuses of the skin, many small nerve fibers branch off, which are responsible for the innervation of skin vessels, hair and glands.
Most of the nerve fibers end in nerve receptors, which are responsible for sensory perception.
The main nerve receptors of the skin are:
- thermoreceptors ( temperature responsive);
- mechanoreceptors ( pressure and stretch receptors);
- pain receptors.
Causes of bedsores
 Bedsores occur in people with limited mobility who are bedridden or wheelchair-bound. They are formed in those places where the greatest pressure is applied to the skin. This is the area of the sacrum, shoulder blades, femur and other areas of the body that are located above the bony protrusions.
Bedsores occur in people with limited mobility who are bedridden or wheelchair-bound. They are formed in those places where the greatest pressure is applied to the skin. This is the area of the sacrum, shoulder blades, femur and other areas of the body that are located above the bony protrusions. Mechanism of bedsore formation
Pathogenesis ( mechanism of disease development) the formation of bedsores comes down to impaired tissue nutrition. This is based on two mechanisms - circulatory disorders and nervous trophism. Together, these two mechanisms are the cause of those metabolic disorders that lead to tissue necrosis.Circulatory disorders develop due to compression of skin vessels, which leads to a decrease in blood supply to this area. Without blood supply, tissue nutrition does not occur. The lack of appropriate nutrients in the cell leads to its death ( necrosis). Disorders of nervous trophism are added to this mechanism. It is known that the nervous system has a regulatory effect on metabolism in organs and tissues. However, in people with limited movements or with their complete absence, there are disturbances in the conduction pathways of the brain or spinal cord ( those violations that led to immobilization). Thus, the disorders nervous regulation, and disturbances in blood supply are the foundation for the development of bedsores. There are many reasons that lead to the development of these two mechanisms.
For example, this is pressure on the corresponding area of the skin, as a result of which the vessels supplying this area are compressed. It is believed that if the two-hour pressure outside exceeds the pressure in the vessels, then the process of formation of bedsores is maximally accelerated. Another reason is excess moisture of the skin, as a result of which it becomes saturated with liquid and swells. This process is called maceration in medicine. As a result, skin damage in the initial stages of pressure ulcer formation is further accelerated.
Most often, several causes are involved in the development of bedsores.
The causes of bedsores are:
- constant friction or pressure;
- multiple concomitant diseases;
- poor patient care, including unbalanced nutrition;
- overweight or underweight.
Constant friction or pressure
Constant friction or pressure is common cause formation of bedsores. This is because bedsores form in areas covering bony protrusions. Thus, the pressure on the skin increases. Being in a stationary position, friction occurs between the surface where the patient lies ( sofa) and bone. As a result of this, the skin with the vessels and nerve endings passing through it is further compressed, and the blood supply deteriorates even more. In the corresponding area of tissue, those pathological processes develop that end in tissue necrosis. Friction can also be caused by folds in sheets or clothing. Any friction or pressure will lead to the formation of microcracks in the skin, which will further increase. Cracks and wounds on the skin of paralyzed patients form much faster, again due to impaired microcirculation. All this leads to redness of the skin at the site of compression. Subsequently, the reddened skin swells.Friction also occurs in cases when exhausted bedridden patients slide out of bed without support in their legs. In this case, a displacement of the superficial layers of the skin occurs in relation to the deep layers. As a result, the smallest vessels of the skin ( capillaries) are torn, and the blood supply to the corresponding areas is disrupted. A similar thing happens when a sheet or blanket is pulled from under a patient.
Multiple comorbidities
This reason affects how quickly bedridden patient Bedsores will develop. Often it determines the outcome of the underlying disease.Concomitant diseases and bad habits that accelerate development of bedsores, are:
- diabetes;
- pathologies of connective tissue and blood vessels;
The most rapidly progressing bedsores develop with atherosclerosis and diabetes mellitus. With atherosclerosis, large vessels are affected, as a result of which the blood supply is disrupted not only at the level of microcirculation, but also macrocirculation. Thus, an atherosclerotic plaque closes the lumen of large vessels, as a result of which a lack of blood supply is observed not in a limited area, but in entire limbs. In diabetes mellitus, in addition to damage to microcirculatory vessels, a general decrease in immunity is observed. As a result, tissue resistance is reduced and the ability to recover is lost. This explains the rapid progression of bedsores in diabetes mellitus and their resistance to all preventive measures.
When smoking, microcirculation is disrupted not only in the vessels of the hands, but throughout the body. This is due to the fact that smokers’ blood is susceptible to increased thrombus formation ( blood clots that block a vessel). This leads to the fact that the smallest blood vessels in the skin quickly become clogged and fail. Compressing such vessels stops blood access to the tissues as much as possible.
Poor patient care, including unbalanced nutrition
Proper care of a paralyzed patient sometimes plays a decisive role in the formation of bedsores. It should include the use of special mattresses, circles, and periodic turning from one side to the other. The skin of patients should be kept clean and free of excess moisture. It is necessary to reduce the pressure on the body as much as possible, as well as reduce irritation. Folds in sheets, clothes and anything that can lead to the formation of microcracks should be avoided. Rough bedding and seams on it, buttons on pajamas - all this increases skin irritation. The situation is aggravated when the patient has urinary or fecal incontinence. In this case, the surface of the sacrum, buttocks, thighs ( most vulnerable surfaces) exposed to excess moisture. The skin begins to get wet, and wounds form on it. The effect is aggravated by the acidic reaction of urine, which has a strong irritating effect. Lack of regular hygiene for such patients leads to accelerated development of bedsores.Kinesitherapy is very important for paralyzed patients. Regular sessions with a kinesiotherapist improve blood flow in paralyzed limbs. If it is not possible to conduct classes, it is necessary to use “air bathing” or light massage. Since treating bedsores is a very long and difficult process, it is much more important to prevent their development. To do this, it is important to turn the patient over daily and monitor his skin. If you don’t do this, you may miss the first signs of bedsores ( swelling and redness).
To reduce pressure, special mattresses, circles, and bolsters are used. All these items increase the area of contact between the body and the surface, thereby reducing pressure on areas of the body. In their absence, the risk of developing bedsores increases, since the pressure on the body is maximum.
Patient care also includes a balanced diet. Nutrition should help restore energy costs. If the protein content in the patient’s food is less than 15 percent, and the patient drinks less than one and a half liters of liquid per day, then the recovery processes in the body are much slower.
Overweight or underweight
With insufficient body weight, patients are usually exhausted. The skin and subcutaneous layers are poorly supplied and nourished. As a result, the slightest cracks and scratches lead to further damage to the integrity of the skin. People who are overweight have a much higher risk of developing bedsore infections. This is due to general hormonal, vascular disorders that develop with obesity.What do bedsores look like?
 Bedsores are dead areas of skin. What these areas look like depends on the stage of development of the bedsores.
Bedsores are dead areas of skin. What these areas look like depends on the stage of development of the bedsores. Stage 1
The area where erosion subsequently forms turns red and swells. There are no visible wounds, only microscopic cracks invisible to the naked eye. Sometimes the skin takes on a bluish or purple tint. Visually, she looks slightly irritated. Patients may notice local soreness.
Stage 2
A superficial wound forms at the site of redness. It looks like a small depression with pink and swollen edges. This wound affects the epidermis and part of the dermis. Sometimes a bedsore can take the form of a burst bubble of fluid, but more often it has the appearance of an ulcer.
Stage 3
At this stage, a deep wound surface is formed. The defect affects all layers of the skin, reaching the subcutaneous fatty tissue. The ulcer takes on the appearance of a deep crater, at the bottom of which there is yellow necrotic tissue. This tissue consists of dead cells of the epidermis and dermis.
Stage 4
The defect extends to deep-lying tissues. At the bottom of the wound, muscles, tendons, joints and even bones are visible.
Also, bedsores can form deep in the soft tissues, but communicate with external environment through a fistula. This is the so-called fistulous form of bedsore. There is only a small hole on the surface of the skin. It communicates with another wound cavity ( actually with a bedsore) through a narrow convoluted channel ( fistula). The bedsore itself appears to be closed. However, it can be located quite deep. From this deep cavity, purulent contents are separated through the fistula onto the surface of the skin. With this form of pressure ulcers, a common complication is osteomyelitis or purulent arthritis.
In bedridden patients, bedsores usually form on the back ( in the area of the shoulder blades), in the area of the sacrum, heels. If the patient lies on his side, then on the femoral surface, on the shoulder, on the knee. In patients who use a wheelchair, bedsores appear on the gluteal region, on the sacrum, and also on the back of the arms.
Which doctor should I contact for treatment?
 Treatment of bedsores is usually carried out by the doctor treating the underlying disease. For example, if a patient is paralyzed due to neurological disease (stroke, spinal cord injury), then this doctor is a neurologist. He gives recommendations for patient care and prescribes treatment to restore blood circulation. As a rule, he collaborates with a kinesitherapist who is involved in the rehabilitation of the patient after an injury or illness. He is both a massage therapist and a specialist in therapeutic exercises. This doctor develops the motor activity of a lying patient. If movements are impossible, then manual therapy or electrical stimulation of paralyzed muscles is recommended.
Treatment of bedsores is usually carried out by the doctor treating the underlying disease. For example, if a patient is paralyzed due to neurological disease (stroke, spinal cord injury), then this doctor is a neurologist. He gives recommendations for patient care and prescribes treatment to restore blood circulation. As a rule, he collaborates with a kinesitherapist who is involved in the rehabilitation of the patient after an injury or illness. He is both a massage therapist and a specialist in therapeutic exercises. This doctor develops the motor activity of a lying patient. If movements are impossible, then manual therapy or electrical stimulation of paralyzed muscles is recommended. The principles of rehabilitation are:
- breathing exercises;
- disembarking the patient;
- passive movements with limbs;
- treatment by position.
However, if deep defects form, then in this case they turn to surgeons. If necessary, he excises the edges of the wound, removing dead and non-viable tissue. It drains ( creates an outflow of pathological fluid from the wound) wound surface, introduces antibacterial drugs there, and also gives advice on further care.
When is inpatient treatment necessary?
Treatment in a hospital is necessary when complications develop, as well as when bedsores of degrees 3 and 4 develop.Complications of bedsores are:
- bone infections ( osteomyelitis);
- infection of subcutaneous fat tissue.
The first signs of sepsis are high fever and chills. At the first such symptoms, you should consult a doctor. The spread of infection to bone tissue is also a serious complication. In this case, the purulent-necrotic process affects both the bone and joints.
Acute infection of the subcutaneous fat tissue requires immediate surgical intervention, as it can provoke sepsis or meningitis.
Ointments and solutions for the treatment of bedsores
There is a large selection of ointments, solutions and special materials for the treatment of bedsores. They are selected depending on the stage of skin damage and the spread of the pathological process to deeper layers. The choice of medications should be made only by the attending physician.Ointments for bedsores
Ointments used in the treatment of bedsores are represented by a large number of drugs from different groups. They have various mechanisms actions and, accordingly, various therapeutic effects.The main therapeutic effects of ointments for the treatment of bedsores are:
- restoration of normal blood circulation to improve skin trophism;
- stimulation and activation of general and local tissue regeneration processes;
- prevention and elimination of the development of bacterial infection in the wound;
- elimination of possible pain syndrome and uncomfortable subjective feelings at the patient.
| Name of ointment | Compound | Mechanism of action |
| Methyluracil |
| Intracellular metabolism is normalized and the skin regeneration process is started. As a result, granulation formation and tissue healing are accelerated. |
| Levosin |
| Enzymes break down all necrotic tissue. Methyluracil has a high wound healing effect, stimulating the regeneration of damaged skin. |
| Levomekol |
| The antibiotic destroys the infection. Methyluracil has a high wound healing effect, stimulating the regeneration of damaged skin. |
| Argosulfan
(dermazin, sulfargin) |
| An antibiotic stops the growth and development of bacteria. Silver ions stimulate skin regeneration. itching, burning). |
| Metrogyl gel |
| An antibiotic stops the growth and development of bacteria. It is especially effective in treating wounds infected with anaerobic bacteria. The foul odor is eliminated and the copious discharge from a pressure wound. |
| Solcoseryl |
| Tissue trophism and intracellular metabolism improves. The processes of skin reparation and restoration are actively stimulated. |
| Zinc ointment (cindol) |
| Affects the inflammatory process, significantly reducing exudation. As a result, the wound dries and a protective covering is formed. Zinc oxide also has a moderate antiseptic effect. |
| Algofin |
| Stops the growth and reproduction of pathogens skin infections. By osmosis, it draws fluid from the wound, reducing exudation and swelling. Actively stimulates skin repair and regeneration. |
| Iruksol |
| An antibiotic prevents and eliminates the development of infection. Enzymes break down all necrotic ( dead) fibers and cells without damaging healthy tissue. By cleansing the wound, its healing speeds up. |
| Betadine |
| Iodine reacts with proteins of bacteria and pathogenic fungi, destroying them. As a result, the infection dies. Iodine also destroys proteins in necrotic tissue, helping to cleanse the wound. |
| Thiotriazolin |
| Thiotriazolin stops the formation of free radicals in necrotic tissue. Thus, it protects epithelial cells from the destructive effects of radicals. The drug also stimulates restoration and regenerative processes in the skin. |
| Bepanten |
| In skin cells, the drug is converted into vitamin B5, which is actively involved in cellular repair processes. |
The choice of ointment depends on the stage of development of the bedsore and the presence of an infectious process.
In the first stage of bedsore development, therapy is aimed at improving blood circulation and tissue trophism. Ointments should also have an antimicrobial effect to prevent the development of infection.
Effective ointments that are used for the first stage of bedsores
- argosulfan;
- dermazin;
- zinc ointment;
- cindol.
If pathogenic bacteria enter the wound and signs of infection appear, ointments containing antibiotics are prescribed. Antibiotics are also indicated in cases of deep necrosis with copious discharge.
Ointments that are used to fight infection
- levomekol;
- argosulfan;
- iruksol;
- levosin.
Ointments that are used for the second stage of bedsores
- iruksol;
- betadine;
- methyluracil;
- Thiotriazoline.
Ointments that are used in the third stage of bedsores
- solcoseryl;
- algofin;
- levosin;
- bepanthen;
- thiotriazoline;
- iruksol.
Solutions for bedsores
Before using ointments, bedsores are treated with disinfectant and antiseptic solutions.| Name of solution | Active substance | Mechanism of action |
| Chlorhexidine bigluconate;
hexicon | chlorhexidine | Provides wound disinfection and destruction of all bacteria. Effective against infection with skin fungi and some viruses. Doesn't have any negative influence on the cells and tissues of the body. |
| Solution with silver compounds (colloidal silver) | silver ions | Silver ions stop the growth and reproduction of bacteria. They also enhance the effect of the antibiotic, eliminate pain and local discomfort ( itching, burning). |
| Furacilin | nitrofural | The active substance binds to the proteins of pathogenic bacteria and changes their configuration. As a result, the cell cannot use its proteins for life and dies. |
Daily care of a patient with bedsores
Patients with limited physical mobility and pressure ulcers require adequate care. Compliance with a number of rules during care will prevent complications and stop the process of necrosis of soft tissues.Factors that need to be provided to a patient with bedsores are:
- reducing pressure on the body;
- organization of proper nutrition;
- ensuring proper skin care.
Reducing pressure on the patient's body
To prevent worsening of the pressure ulcer process, it is necessary to reduce the pressure on the patient’s skin. There are a large number of devices to support individual parts of the body and to distribute pressure evenly.Devices that may be used when caring for a patient with pressure ulcers include:
- mattress pads;
- gel pillows;
- linings made of soft materials;
- mattresses against bedsores.
Nutrition and drinking of patients with bedsores
The patient's diet must be balanced and complete, taking into account the restrictions given by the doctor ( if they exist). A prerequisite for rapid healing of bedsores is compliance with the recommended daily amount of protein, which is equal to 20 percent ( approximately 120 grams) from the total volume of food. Also, the diet should provide the patient with sufficient amounts of vitamin C and elements such as iron and zinc. The amount of liquid consumed, if there are no contraindications, should be no less than 1.5 liters. The consistency of the dishes should be liquid, mushy or semi-solid. The food temperature is medium, and the number of meals is at least 5.- broths from fish, lean meat, vegetables;
- porridge;
- cottage cheese casseroles;
- steamed omelettes;
- steam cutlets and meatballs;
- vegetable purees;
- milk and vegetable soups.
Principles of proper skin care for bedsores
Providing comprehensive, competent care for the skin of a patient with pressure ulcers will speed up wound healing and prevent the formation of new areas of tissue necrosis.The goals of skin care for a patient with pressure ulcers are:
- reduction of irritation;
- maintaining cleanliness;
- prevention of secondary infections and aggravation of pressure ulcers.
Limiting skin irritants
To reduce the level of irritation, it is necessary to use bedding made of soft fabrics, on the surface of which there are no rough seams, patches, zippers, or buttons. The bed needs to be straightened out from wrinkles frequently and ensure that there are no crumbs or various small objects in it. Urine and feces are strong irritants, so toileting of the perineum should be performed after each act of defecation or urination. For incontinence, pads or special diapers should be used. In some cases, urine bags may be used ( for men with incontinence). Sweat also has a strong irritating effect on the skin, so you should carefully maintain the patient’s hygiene, change his clothes and bed linen. It is recommended to replace bedding and underwear along with changing the patient's body position. To reduce the intensity of sweating, it is necessary to provide the patient with a comfortable temperature regime and prevent overheating of the body. The patient and caregiver should keep their nails short to prevent scratching or accidental injury.Rules for carrying out hygienic measures when caring for patients with bedsores
Insufficiently clean skin is a favorable factor for the development of pressure ulcers. Therefore, the hygiene of a person with tissue necrosis should be given sufficient quantity attention and perform all stages of care ( cleansing, protection, moisturizing). When carrying out water procedures, you should not use hard washcloths and rough towels, strong-smelling or brightly colored detergents. Water can also cause discomfort for the patient due to the various microelements it contains, so the interaction of the skin with water should be minimized. Special products and devices will help provide all the requirements for proper skin care for bedsores. Such products have a gentle effect on the skin and provide effective protection.Skin hygiene products are:
- emulsions that allow you to cleanse your skin without water or soap ( No Rinse washing gel, Seni cleansing foam);
- means for preventing diaper rash ( powders, talc);
- moisturizers ( Healing Derm balm, Menalind lotion);
- healing creams ( Convin Kritik Barrier cream, Badyaga gel, Ambulance balm for wounds);
- preparations for the care of the skin of the perineum when using diapers ( Sudocrem, Bepanten, skin protector Menalind);
- foaming sponges and mittens for water procedures ( Cleanet, Gantnet plus, Ninonet).
Prevention of infections
To prevent the progression of pressure ulcers, potentially dangerous places ( where bedsores can occur) are treated with camphor alcohol, a solution of vinegar and water, or ammonia diluted with water in a ratio of 1 to 4. In some cases, bedsores are accompanied by secondary infections, and the skin needs to be treated with antiseptic and antibacterial agents prescribed by the doctor.How to make dressings?
An important component of bedsore treatment is dressing. There are several basic conditions that bandages must meet.The dressing for the treatment of bedsores must meet the following parameters:
- be sealed to prevent infection;
- be dense ( 8 – 10 gauze layers);
- be breathable;
- the area of the dressing should exceed the area of the wound;
- The edges of the bandage are attached at the level of healthy skin.
The bandage should not be too tight and block the flow of oxygen to damaged tissues. To bandage a patient with bedsores, it is necessary to prepare some tools and materials, as well as have appropriate ointments and antiseptic solutions.
The necessary materials for dressing are:
- sterile wipes;
- tweezers;
- scissors;
- gloves;
- dressing material ( gauze, bandage, special plates);
- patch;
- ointment and antiseptic solution.
Before treating and applying a bandage to a bedsore, it is necessary to assess the condition of the skin. The choice of ointment and dressing material depends on the stage of the pathogenic process.
Dressing includes four main points:
- opening of a wound;
- treatment with an antiseptic solution;
- applying ointment;
- gluing the bandage.
The bandage should be larger than the area of the wound itself, so that its edges are on healthy areas of the skin. The bandage is glued around its entire perimeter with a plaster. If frequent use of the patch causes swelling and redness of the skin, you should switch to a hypoallergenic patch. When bedsores form in the heel, elbow and knee joints, the bandage is secured with a bandage.
Currently, there are many special dressing materials for effective treatment bedsores. These materials are impregnated with various medications that promote rapid wound healing.
Special dressing materials
| Material | Compound | Characteristic |
| Alginate dressings | Sterile seaweed dressing. | Absorbs liquid quickly and efficiently. Indicated for the treatment of infected bedsores with copious purulent discharge. |
| Hydrocolloid dressings | Multilayer dressing impregnated with a special substance. | When exposed to wound secretions, the substances in the dressing turn into a gel. The gel absorbs exudate and purulent discharge. |
| Hydrogels | Napkins or plates soaked in gel. | The gel helps soften dead tissue and facilitate its easy rejection. |
| Gauze dressings with various active enzymes | Sterile dressings coated with enzymes. | Active enzymes break down all necrotic tissue. Intracellular metabolism is normalized and the skin regeneration process is started. |
These materials are sold in sterile packages. They come in various shapes and sizes. Some of the materials are applied to the site of the bedsore, covered with gauze pads and glued with a plaster. But most of them have a fabric backing that adheres to the skin.
How to treat bedsores with antiseptics?
Bedsores should be treated only with gentle antiseptics that do not cause burns to viable tissues and do not slow down their regeneration. Chlorhexidine, furatsilin and silver solutions are considered harmless antiseptic solutions. There are several rules for treating bedsores with antiseptics.The main rules for treating bedsores with antiseptic solutions are as follows:
- Do not touch the wound surface with your hands, but only with sterile napkins;
- do not overuse antiseptic solutions;
- exclude the use of iodine, brilliant green, hydrogen peroxide and potassium permanganate.
- the solution is applied to sterile wipes or to the wound directly from the bottle.
How to treat a wound with healing drugs?
At the healing stage of a bedsore, it is important to prevent tissue softening and stimulate regeneration processes. For this purpose, various preparations are used in the form of ointments and special materials for dressings.Healing drugs for the treatment of bedsores include:
- ointments with silver ions ( );
- complex ointments containing active enzymes ( levosin, levomekol);
- methyluracil ointment;
- solcoseryl ointment;
- algofin ointment
- dexpanthenol ( bepanten);
- special materials impregnated with active enzymes ( multitruss and comfil coatings).
Method of using healing drugs
| A drug | Mode of application |
| Ointments with silver ions (argosulfan, dermazin, sulfargin) | A thin layer of 2 - 3 millimeters is applied to the wound up to three times a day. |
| Complex ointments containing active enzymes (levosin, levomekol) | The ointment is applied daily to the wound surface, completely filling the tissue defect. A bandage is applied on top. |
| Methyluracil ointment | Apply a thin layer ( up to 10 grams) on a wound or bandage. The frequency of dressing changes depends on the condition of the wound ( on average 1 – 2 times a day). |
| Solcoseryl ointment | Apply a thin layer of ointment to the wound twice a day. Initially, a 25 percent ointment is applied. Then it is replaced by 5 percent. |
| Dexpanthenol (bepanten) | Dexpanthenol in the form of a spray is applied to the bedsore 3 – 4 times a day. Dexpanthenol ointment ( bepanten) is applied in a thin layer to the wound 2 – 3 times a day. |
| Special materials impregnated with active enzymes (multitruss coverings, comfil) | Special materials are selected according to the size of the bedsore. When the wound is clean and dry, the material is applied without prior application of ointments. At the initial stage, multitruss and polytruss coatings are used. The dressing is changed every 24 to 48 hours. Then they switch to economical comfil coatings, which can be changed less frequently ( once every 3 – 4 days). |
Physiotherapy for bedsores
Physiotherapy is included in the complex of therapeutic measures for bedsores. The choice of method depends on the goals of treatment, which are determined by the stage of the necrotic process.At the initial stage of development of bedsores, physiotherapy is prescribed to improve blood circulation and eliminate primary symptoms.
| Procedure name | Method of implementation | Achieved effect | Systematic implementation |
| Shock wave therapy (UVT) | This therapy is carried out using a device that generates sound waves of a certain frequency, which are directed to the affected areas of the body. The acoustic effect is carried out by a special sensor, which is located on areas with bedsores. | Sound vibrations provide micro-massage to tissues, which improves blood circulation in the affected areas and reduces swelling. | The device settings and session duration are determined by the doctor individually. The pause between procedures should be at least a week. The duration of treatment is from 5 to 7 doses. |
| Magnetotherapy | The principle of therapy is the influence of a constant or pulsed magnetic field on the lesions. | The influence of magnets improves blood and lymph circulation, has an anti-inflammatory effect and accelerates the process of restoration of damaged tissues. | The course of therapy consists of 5–10 procedures, the total duration of which varies from 100 to 200 minutes. |
| Darsonvalization | During the procedure, alternating current is applied, the intensity of which varies from weak, imperceptible discharges to spark pulses that cause noticeable skin irritation. | The consequence of darsonvalization is improved tissue nutrition, stimulation of metabolic processes, and normalization of blood circulation. | At the beginning of the session, various movements are carried out with the electrode at a distance of 3 to 6 millimeters from the skin in a zone of 5 to 8 centimeters from the wound for 3 to 5 minutes. Then the emitter is moved directly to the lesion for 1 - 3 minutes, maintaining an air distance. Full course Darsonvalization is equal to 10 – 15 sessions. |
At the stage of necrosis, the goal of physiotherapy is to fight infection and cleanse wounds of necrotic formations.
| Procedure name | Method of implementation | Achieved effect | Systematic implementation |
| Electric field (UHF) | Capacitor plates are applied to the affected areas, through which AC pulses are applied. electric current with ultra-high frequency. | The electric field helps to dilate blood vessels, normalize tissue nutrition processes, and increase the activity of barrier cells. | The impact is carried out on the area next to the bedsores in doses of 15 - 20 watts every day. The minimum duration of therapy is 5 procedures, the maximum is 15. |
| Ultraviolet irradiation (Ural Federal District) | Treatment is carried out using a mercury-quartz lamp and is prescribed for pressure wounds and the skin around them. The ultraviolet rays used can be long-wave, mid-wave or short-wave. | Irradiation helps fight inflammatory processes, stimulates immune function and has an analgesic effect. | In the presence of extensive necrosis, therapy begins with three biodoses ( duration of radiation at which skin redness occurs). With each subsequent procedure ( The course is assigned from 8 to 12) the duration of irradiation is increased by half the biodose. If the granulation process is delayed or wet surfaces predominate on the wounds, 20 to 30 sessions are prescribed, the duration of which varies from 0.5 to 1 biodose. |
| Ultrasound therapy | The treatment principle is based on the use of ultrasonic vibrations. Using a radiator, the doctor makes slow stroking movements over the affected areas. To ensure contact between the body and the sensor, the skin is treated with a contact gel. | Under the influence of ultrasound, various processes are initiated in tissues that help the body fight infection. The therapy has a pronounced analgesic and tonic effect. | The duration of one session should not exceed 15 minutes. The treatment course may include from 7 to 15 procedures. |
| Electrophoresis of antibiotics and antifungal drugs | The therapeutic effect is achieved through the effect of direct current on the body, which increases the effect of medications. A cloth pad is moistened with the medicine and placed on the wound. A metal electrode is installed on top, which conducts electrical impulses. | Electrophoresis makes it possible to increase the effectiveness of drug treatment with fewer drugs. This type of therapy also reduces the likelihood of side effects. | |
| Franklinization | Electrotherapy in which the patient is exposed to local high voltage electrical current using plate-shaped electrodes. The therapeutic effect is enhanced by the action of ozone, air ions and nitrogen oxides, which are formed during discharges. | This physiotherapy is prescribed when there is a large amount of pus in the wound, as it has a strong bactericidal effect. | The duration of the session depends on the product used and can vary from 5 to 20 minutes. The therapeutic course is equal to 15 – 20 procedures. |
During the regeneration stage, physiotherapy procedures are prescribed to accelerate healing and restore disturbed physiological processes in wounds.
| Procedure name | Method of implementation | Achieved effect | Systematic implementation |
| Treatment with sinusoidal modulated currents (SMT) | The essence of the procedure is the effect of weak alternating current on pressure ulcers. This method of physiotherapy has a long-lasting effect, as the impulses penetrate deep into the tissue. | Sinusoidal currents, by their action, activate physiological processes in the affected tissues, thereby accelerating wound healing. | The patient is prescribed 7 to 10 procedures, which are performed every day. |
| Phonophoresis | Treatment consists of the combined effects of drugs and an ultrasound field. The drug is applied to the skin, after which the doctor makes light movements over the treated area using a sensor. | Therapy sessions last from 10 to 30 minutes and are carried out at intervals of 2 days. The course of treatment ranges from 10 to 15 procedures. | |
| Ozokerite | Heated ozokerite ( mountain wax) is applied in the form of compresses or formed cakes according to the size of the wound. The top of the applique is fixed wax paper, oilcloth and blanket to create a thermal effect. | This therapy has a regenerating effect, improving blood circulation and delivery of nutrients to affected tissues. Microelements provide additional beneficial effects ( calcium, iron, manganese), which are part of ozokerite. | Mountain wax is applied for 30 – 40 minutes. After removing the ozokerite, the affected area is covered with a blanket for half an hour. Treatment sessions are carried out every other day with a course of 15–20 procedures. |
How to choose a mattress for the prevention of bedsores?
In the treatment of bedsores, as well as for the purpose of their prevention, special mattresses are widely used. These products differ in functionality, design features and other characteristics. The choice of mattress depends on the patient’s weight, the nature of the bedsore process and the patient’s degree of mobility.Parameters to consider when purchasing a mattress are:
- functionality ( dynamic or static);
- type of material;
- product type ( cellular or tubular);
- presence of microventilation;
- compressor characteristics;
- load capacity and dimensions of the anti-decubitus system.
Static or dynamic mattress
A static mattress is a product whose surface is stationary. The device takes the shape of the patient’s body, which ensures uniform pressure distribution and reduces the likelihood of bedsores. Such mattresses are suitable for partially mobile patients who require bed rest.The surface of a dynamic mattress is in constant motion, due to which the body of the person lying on it is subjected to continuous massage. It is advisable to purchase such products for patients who cannot move independently.
Types of materials from which anti-decubitus mattresses are made
Orthopedic mattresses are made from polyurethane foam or polyvinyl chloride ( PVC). PVC products are easy to use, easy to clean, do not absorb liquid and are suitable for patients who suffer from urinary or fecal incontinence. Polyurethane foam mattresses allow air to pass through better and have a thermoregulating effect. Even when lying on them for a long time, patients do not experience discomfort due to overheating or fogging. Such mattresses are more effective in combating bedsores, and are also suitable for patients with frequent fevers.Tubular and cellular mattresses
Depending on the design features, dynamic mattresses can consist of tubular or cellular sections. The choice of structure depends on the stage of tissue necrosis and the weight of the patient.A cellular mattress is a canvas made of diamond-shaped or square sections, which are filled with air in a certain order and deflated with a break of 5 to 12 minutes. Thanks to constant change of body support and massage, blood circulation and tissue nutrition improves. Such mattresses are suitable for preventing tissue necrosis and treating the initial stages of this process. Also, these products are suitable for patients whose weight does not exceed 120 kilograms.
Patients who have bedsores of the second, third and fourth stages should purchase tubular mattresses. Such devices are also recommended for those people who weigh more than 120 kilograms. The products consist of hollow tubes arranged transversely, which are alternately filled with air. The increased size of the chambers, compared to a cellular mattress, promotes more effective tissue massaging and reduces pressure on the affected areas.
Airflow system
Some mattress models have a special coating, the surface of which is perforated using a laser. Micro-holes promote high-quality air exchange, due to which the patient’s skin gets rid of excess moisture. Such products are recommended for patients who are overweight or have excessive sweating.Compressor type
All dynamic mattresses are equipped with compressors that supply air to the hollow sections. When purchasing a product, you should take into account the noise level that the motor produces during operation. The recommended noise range ranges from 5 to 10 decibels. Higher noise levels may adversely affect the patient's well-being.Dimensions and maximum permissible weight of the mattress
Load capacity and dimensions of the mattress ( indicated by the manufacturer in the technical specifications of the product) are determined by factors such as bed parameters and patient weight. The maximum weight that the product can support must exceed the weight of the patient, otherwise the body will come into contact with the surface of the bed at points of maximum pressure. The length and width of the mattress should be identical to the dimensions of the bed.In order to understand the best way to treat bedsores, you need to have an idea of the causes of this problem. What causes damage to the skin and underlying tissues in bedridden patients?
Reasons for the development of bedsores
The key factor is pressure of the hard surface on which the patient is located on protruding areas of the body. Most often, injuries occur in areas such as the sacrum, thoracic spine, shoulder blades, back of the head, heels (in situations where a person lies on his back) - it is in these areas between the bone tissue and skin that there is a very small layer of muscle and fatty tissue.
When the patient lies on his side, the greatest pressure falls on the areas greater trochanter femur, ilium. In the prone position, the tissues in the areas of the protruding iliac bones and chest are damaged. In sedentary patients, the risk of injury is higher in the area of the ischial tuberosities, sacrum, heels, fingers, feet, and shoulder blades.
Why does pressure cause damage to tissue?
- Blood vessels are compressed, ensuring the delivery of oxygen and nutritional components to skin and muscle cells. Oxygen starvation (hypoxia) and nutritional deficiency lead to inhibition of cell activity and its death;
- Nerve fibers are compressed, regulating metabolism in tissues: which, in turn, negatively affects cell viability
- Lymphatic vessels are compressed, responsible for removing cell waste products from the intercellular space, waste and poisons begin to accumulate, reducing the viability of cells and leading to their death as a result of poisoning. The lymphatic system is also responsible for the removal (disposal) of dead cells: compression of the lymphatic vessels leads to the accumulation of dead cells in the tissues - and this creates favorable conditions for the development of infection
Stages and types of bedsores
In the process of caring for a bedridden patient, it is very important to know what types and stages of damage there are when it comes to such a problem as bedsores in bedridden patients, and the question arises - how to treat it at home? In the photo you can see what bedsores look like in various stages.
There are four stages of development of pressure ulcers:

It is very important to notice the first signs of damage development in time, best when they are still reversible. In a situation such as bedsores, the initial stage, minimal treatment is required. The photo shows that there is no damage to the skin yet, and it is enough to eliminate the harmful factors to stop the dangerous process.
Bedsores are also divided into exogenous - caused primarily by external factors, endogenous - their occurrence is associated primarily with disorders within the body, and mixed - appear under the influence of both external and internal factors.
Endogenous bedsores very often occur in patients with disorders of the nervous system (traumas and tumors of the brain and spinal cord, cerebral hemorrhages), as well as with metabolic disorders (for example, diabetes mellitus). In this case, disorders of the nervous regulation of metabolic processes in tissues occur, so the development of damage often occurs from the inside out: that is, damage to muscle tissue develops first, and only then signs on the skin become noticeable.
 When it comes to a problem such as bedsores, treatment at home should be comprehensive and include the following areas:
When it comes to a problem such as bedsores, treatment at home should be comprehensive and include the following areas:
- Measures to eliminate the factors that caused the development of bedsores,– pressure, friction, displacement, excessive moisture;
- Local treatment, which (depending on the stage) can be aimed at improving blood circulation in the affected area, eliminating irritation, fighting infection with local funds, acceleration of healing processes, etc.
- Taking general and systemic drugs(orally, intramuscularly, intravenously), aimed at fighting infection, improving metabolic processes, blood circulation, etc.
- Treatment of the underlying disease, which led to limited mobility and caused the development of bedsores (especially important in the case of endogenous bedsores resulting from internal disorders).
In general, treatment tactics are determined by the stage of the process and the depth of tissue damage, as well as the presence of infectious complications.
Measures to eliminate the factors that led to the development of bedsores
How to reduce pressure on tissue to avoid cell death (in the initial stage) and prevent the spread of necrosis to deeper tissues? To solve this problem, the following measures are proposed:
- regular changes in the patient’s body position;
- use of special circles and pillows;
- use of anti-decubitus mattresses.
Changing body position
 Regularly changing the body position of a bedridden patient can reduce the load on areas subject to the greatest pressure. This makes it possible not only to avoid progression of the process with existing bedsores, but also to prevent the appearance of new damage.
Regularly changing the body position of a bedridden patient can reduce the load on areas subject to the greatest pressure. This makes it possible not only to avoid progression of the process with existing bedsores, but also to prevent the appearance of new damage.
The Protocol for the management of patients with pressure ulcers (recommendations of the Ministry of Health of the Russian Federation for the treatment and prevention of pressure ulcers) states that in areas of increased risk of developing injuries (which we discussed above) changes in tissues leading to cell death can begin after just two hours of continuous pressure. This is especially true for patients with injuries and diseases of the nervous system, metabolic and vascular disorders. Because in such situations, the effect of an external factor (pressure) is aggravated by the influence of internal factors (tissue nutritional disorders).
That is why it is recommended to change the body position of a lying patient at least every two hours throughout the day (including night time). There are several special positions that minimize pressure on tissue in risk areas: the Sims position, the side-lying position, the prone position, and the Fowler position. Certain techniques have been developed for moving a bedridden patient to each of these positions:
Move to Sims position

Moving to the side-lying position

Moving to the “Lying on your stomach” position

Placement in Fowler's position
 This position allows the recumbent patient to be in a semi-sitting position, which makes breathing, eating, communication easier and is psychologically comfortable for him. To place the patient in this position, a bed with a raised head end (functional bed) is best suited, but special pillows can be used.
This position allows the recumbent patient to be in a semi-sitting position, which makes breathing, eating, communication easier and is psychologically comfortable for him. To place the patient in this position, a bed with a raised head end (functional bed) is best suited, but special pillows can be used.
- The patient is moved to the supine position: you can choose a position at an angle of 45 (low Fowler position) or 60 (high Fowler position) degrees;
- Pillows are placed under the patient’s head, lower back, elbows, hips, and lower third of the leg.
- A support is placed under the patient’s feet to prevent the patient from sliding, which leads to tissue displacement in the sacral area.
With each movement, it is recommended to examine the patient’s body both in the area of existing bedsores (to assess their condition) and in areas where there is a risk of new injuries. The video will help you get acquainted with the algorithm of actions when changing positions of a bedridden patient:
It is most convenient to carry out manipulations to change the body of a patient located on a functional bed specially adapted for the care of patients with limited mobility.

Purchasing a functional bed for caring for a bedridden patient at home seems especially appropriate when it comes to patients bedridden for a long time (months and years). When placing a patient on a regular bed, a number of conditions must be met.
The Protocol for the care of patients with pressure ulcers indicates inadmissibility of placing the patient on a bed with armored mesh or a mattress that causes areas of the patient’s body to “sag” (which impairs blood circulation), making it more difficult to care for the patient, change body position, etc. It is also important that the bed is not too low: it is optimal if the patient is at the level of the middle thighs of the person performing care. A position that is too low makes manipulation difficult and can lead to errors in care.
Using special pillows
A pillow and a circle for bedsores are devices that help reduce pressure on tissues in areas of increased risk of developing damage, avoiding friction and tissue displacement. In addition, they create a more comfortable bedside environment for patients with limited mobility.
We have already mentioned how pillows are used for bedridden patients against bedsores in different positions of the patient in bed. Now let’s take a closer look at the types of pillows and circles, talk about which products are best to choose and how you can make such devices with your own hands.
Pillows differ in shape, material from which the surface is made, and also filling. What types of pillow shapes are there?

 Surface of pillows It can be flat (smooth) or have a certain relief - rough, cellular, etc. In the second case, in addition to the effect of reducing pressure on the area of the bedsore (or the place of its potential development), the blood supply in the risk zone is stimulated: a kind of micro-massage is performed.
Surface of pillows It can be flat (smooth) or have a certain relief - rough, cellular, etc. In the second case, in addition to the effect of reducing pressure on the area of the bedsore (or the place of its potential development), the blood supply in the risk zone is stimulated: a kind of micro-massage is performed.
Types of fillings for pillows: foam rubber, latex, gel, foam (polyurethane foam). Can also be used as a filler air(inflatable pillows). When using them, you can control the amount of injected air, and, therefore, the degree of elasticity. Such pillows can consist of one section or of many cells connected to each other. In the second case, air flows from one cell to another, which creates opportunities for uniform pressure distribution.
On the Internet you can find information about the use of such fillers as millet, flax, buckwheat, etc. in pillows. For example, it is believed that they can be used to make such a device as a bedsore pillow with your own hands. However, unlike gel, foam, latex and other fillers, which have the ability to reduce and redistribute pressure and take the shape of the patient’s body, fillers made from cereals and seeds are very hard and do not adapt to the contours of the patient’s body. As a result, their use may increase pressure in risk areas, increasing the risk of injury.
 Bedsore circles can also be used to relieve pressure - the photo shows that they come in different sizes. Circles with a diameter of up to 30 centimeters are intended for placing under the head, elbows, shins, and heels. To prevent damage to the buttocks and tailbone area, a circle with a diameter of 40 cm is suitable. Circles with a larger diameter are intended for use in obese patients.
Bedsore circles can also be used to relieve pressure - the photo shows that they come in different sizes. Circles with a diameter of up to 30 centimeters are intended for placing under the head, elbows, shins, and heels. To prevent damage to the buttocks and tailbone area, a circle with a diameter of 40 cm is suitable. Circles with a larger diameter are intended for use in obese patients.
Bedsore pads are made of rubber; air is used as a filler, and less often, water. It is recommended to place them in a pillowcase or under a sheet before use to avoid irritation where the skin comes into contact with the rubber.
Sometimes relatives caring for a bedridden patient ask the question - how to make a circle for bedsores with your own hands? In reality, it is quite difficult to make a rubber circle yourself. It is not advisable to use gauze or fabric to make it (such recommendations can be found on the Internet), since these dense materials can increase pressure at the points of contact with the skin and lead to new damage.
Anti-bedsore mattresses for bedridden patients
An anti-bedsore mattress is considered an effective means of preventing and treating tissue damage in bedridden patients. Exist different kinds mattresses, the choice depends on the degree of tissue damage, the severity of the patient’s condition, his weight, etc.
For example, you can use foam mattresses, the recommended thickness is 10 cm. A foam mattress is one of the so-called static mattresses for bedsores. They contribute to the uniform distribution of the patient’s body pressure over the surface, but do not have a noticeable additional effect on the tissues. From modern materials For the manufacture of static mattresses, the same materials are used as for pillows - foam, gel, latex.
 It is considered more effective to use the so-called dynamic mattresses– their use is recommended for patients with existing bedsores, a high risk of their development, for patients whose mobility is limited for a long time. Such mattresses not only help to evenly distribute body pressure, but also provide a constant additional massage effect on the tissue.
It is considered more effective to use the so-called dynamic mattresses– their use is recommended for patients with existing bedsores, a high risk of their development, for patients whose mobility is limited for a long time. Such mattresses not only help to evenly distribute body pressure, but also provide a constant additional massage effect on the tissue.
The filler for dynamic mattresses is air - it is pumped into them using a special compressor, which is attached to the mattress. The amount of air depends on the patient’s body weight - the heavier the patient, the less air should enter the mattress, otherwise elasticity will decrease, air will not be able to move freely through the compartments, and pressure on the tissue will increase. Dynamic mattresses are not placed directly on the bed, but are placed on top of the main mattress.
There are two types of dynamic mattresses: cellular and balloon. Cellular mattress against bedsores consists of many small compartments - cells, between which air can move freely. This mattress is a suitable option for patients who are not obese and with minor tissue damage (stage 1-2).
 In balloon (or tubular) mattresses air is pumped into cylinders (sections) located transversely to the patient’s body. There is an alternating change in pressure in each section, which provides a massage effect and improves blood circulation in the tissues. Balloon mattresses are suitable for patients with large body weight (usually Weight Limit the patient for whom the mattress can be designed is indicated in its characteristics), as well as with stage 3-4 bedsores.
In balloon (or tubular) mattresses air is pumped into cylinders (sections) located transversely to the patient’s body. There is an alternating change in pressure in each section, which provides a massage effect and improves blood circulation in the tissues. Balloon mattresses are suitable for patients with large body weight (usually Weight Limit the patient for whom the mattress can be designed is indicated in its characteristics), as well as with stage 3-4 bedsores.
Reduce friction– an important task when caring for patients with pressure ulcers. In order to avoid additional tissue injury, it is necessary:
- Correctly change bed linen (do not pull the sheet from under the patient, but lift him above the bed or roll the patient onto a clean sheet);
- Avoid friction when performing hygiene procedures, do not use bar soap, replacing it liquid means. At the end of the procedures, dry the patient's skin by blotting.
- Regularly inspect the patient's bed, eliminate folds in bed linen, crumbs and other foreign objects.
- Ensure that the patient’s clothing is free of buttons and rough seams. which can injure the skin.
Measures for eliminating excess humidity, which also increases the risk of developing pressure ulcers, should include:
- Usage bed and underwear made of cotton fabrics ensuring sufficient gas exchange. Underwear made from synthetic fabrics increases sweating and increases skin moisture;
- Usage disposable diapers with urinary and/or fecal incontinence. Diapers must be changed every four hours (regardless of the frequency of urination), as well as immediately after bowel movements (bowel movements), followed by hygiene measures;
- Maintaining the room where the patient is located optimal microenvironment– the air temperature should not exceed 18-20 degrees Celsius, because the patient's stay in a hot room promotes sweating and increases skin moisture.
 How are bedsores treated in bedridden patients at home? The choice of agents that have a local effect on the affected area depends on the stage of the process, the depth and extent of necrosis (the area of cell death), as well as the presence of purulent complications.
How are bedsores treated in bedridden patients at home? The choice of agents that have a local effect on the affected area depends on the stage of the process, the depth and extent of necrosis (the area of cell death), as well as the presence of purulent complications.
So, if we are talking about a problem such as bedsores (stage 1), treatment should be based, first of all, on eliminating the factors that caused the damage: measures related to reducing pressure, humidity, and friction have already been mentioned earlier. Since at the initial stage the integrity of the skin is not compromised (the vital activity of cells is inhibited, but death has not yet occurred), the risk of developing infectious complications is low, the use of healing agents and topical antibiotics will not be relevant. To achieve a favorable result - preventing cell death - the use of drugs that activate blood circulation in the damaged area will help.
When cell death occurs (necrotic changes) and there is a violation of the integrity of the skin (stage 2 bedsores), treatment should include topical drugs that stimulate tissue repair (regeneration), anti-inflammatory drugs, local antibiotics, etc.
It is important to remember that before using this or that medicine for bedsores for bedridden patients, you must consult with your doctor.
The table below presents various drugs for bedsores for bedridden patients (local action) and also indicates the goals to be achieved by the use of these drugs. The information provided corresponds to the recommendations of Dr. med. Professor M.D. Dibirov (Department of Surgical Diseases and Clinical Angiology of A.I. Evdokimov Moscow State Medical University).
|
Purpose of using local remedies |
Drugs (or groups of drugs) |
|---|---|
|
Improving blood circulation in tissues, activation of metabolic processes, cell regeneration |
Actovegin, Solcoseryl, Methyluracil, Bepanten |
|
Elimination of dead cells |
Necrolytic drugs (helping to eliminate foci of necrosis), which include enzymes: collagenase, trypsin, etc. |
|
Preventing the development of infection and combating purulent complications that arise |
Local antibacterial and antifungal agents |
|
Reduction of inflammatory manifestations in the lesion |
Local steroidal anti-inflammatory drugs (contain substances similar to adrenal hormones that have the ability to relieve inflammation) |
Also, one of the tasks that the treatment of necrosis of the skin and soft tissues with medications should be aimed at is the elimination of excess fluid that forms as a result of inflammation in the pressure wound. For this purpose, ointments containing zinc can be prescribed. These agents help reduce inflammatory manifestations, “dry” the wound, and have some antimicrobial effects.
In the work “Bedsores. Prevention and treatment” Professor M.D. Dibirov points out that already in the early stages of development of the injury, it is necessary to clean the injury site daily (rinse the area where the bedsore occurs) in order to reduce the risk of infection. However, for these purposes It is not recommended to use products containing iodine and chlorine(including alcohol solution of iodine, chlorhexidine, etc.).
This is due to the fact that these drugs act aggressively, disrupt the permeability of cell membranes, exacerbating metabolic disorders, and can also destroy immune cells that have migrated into the wound to destroy foreign microbes. According to the professor, it is recommended to use ordinary saline solution to treat the wound (it can be prepared at home: 1 tsp of salt per 1 liter of water). After finishing the treatment, the damaged area must be thoroughly dried (by blotting, without rubbing).
Dressings for bedsores
Also Professor M.D. Dibirov believes that for a problem such as bedsores (initial stage), it is recommended to include the use of bandages in treatment. For minor damage, the best option is polyurethane film dressings, which have a “second skin” effect: they do not block air access to the affected area and do not prevent the evaporation of moisture from the surface of the skin. At the same time, such dressings provide protection from mechanical damage and from external pathogens. They are transparent, which makes it possible to observe changes in the damaged area without injuring the wound.
Bandages are effective remedies for bedsores at home, especially those that, in addition to the main effect (protection from damage and infection), have additional medicinal properties, – so-called interactive dressings.
When deciding how to treat bedsores at home using bandages, you must remember that the use of traditional dressings (gauze, bandages) is not recommended, as they can increase skin damage due to friction. They have the ability to “stick” to the wound, which will lead to additional injury during dressing.
 In addition to the use of local remedies, the attending physician may prescribe one or another medicine for bedsores at home, which has a general effect on the body. First of all, we are talking about drugs whose action is aimed at treating the underlying disease. This is especially true for situations where the occurrence of damage to the skin and underlying tissues is caused not only by external, but also by internal factors, which were mentioned above.
In addition to the use of local remedies, the attending physician may prescribe one or another medicine for bedsores at home, which has a general effect on the body. First of all, we are talking about drugs whose action is aimed at treating the underlying disease. This is especially true for situations where the occurrence of damage to the skin and underlying tissues is caused not only by external, but also by internal factors, which were mentioned above.
Drugs may be prescribed that improve metabolic processes in nerve and muscle tissue, stimulate blood circulation, vitamin complexes. The use of B vitamins, as well as ascorbic acid - vitamin C, is especially important.
It is also important to understand that pressure wounds are an entry point for pathogenic microbes. If an infection occurs, the doctor may prescribe antibiotics for bedsores orally (orally, intramuscularly, intravenously) along with local antibacterial agents.
It is necessary to remember what about a problem like purulent bedsores, treatment at home may be unsafe. Many bedridden patients have a weakened immune system, so the infection quickly spreads to surrounding tissues, leading to inflammation in other organs. In addition, there is a high risk of developing sepsis (blood poisoning) - a deadly complication!
Therefore, only the attending physician can correctly determine the tactics for managing a patient with bedsores in the event of a soft tissue infection: antibiotics (for local and general treatment), hospitalization of the patient, surgical intervention - the sooner adequate measures are taken to treat infectious complications, the higher the likelihood of a favorable outcome.
 When answering the question “how to cure bedsores in a bedridden patient at home,” you must remember the role of good nutrition as important condition solutions to this problem. Thus, for the restoration processes (regeneration) of tissues to occur in the damaged area, that is, the construction of new cells, a sufficient amount of protein must be supplied to the body.
When answering the question “how to cure bedsores in a bedridden patient at home,” you must remember the role of good nutrition as important condition solutions to this problem. Thus, for the restoration processes (regeneration) of tissues to occur in the damaged area, that is, the construction of new cells, a sufficient amount of protein must be supplied to the body.
In addition, people forced to lead a sedentary lifestyle develop muscle atrophy - a decrease in the mass and volume of muscle tissue, which leads to a further decrease in overall tone, progression of microvibration deficiency, etc. Protein foods will provide the body with the building materials necessary for tissue repair.
According to the Protocol for the management of patients with pressure ulcers, the diet of a patient with limited mobility should include at least 120 g of protein daily, which can be obtained from both animal (meat, fish, poultry, milk and dairy products) and plant (nuts, legumes, etc.) products.
It is also important that the diet is rich in vitamins, primarily vitamin C, which is necessary for the full functioning of the immune system (which is important for the prevention of infectious complications). Recommendations for the management of patients with pressure ulcers indicate that The daily dosage of ascorbic acid (vitamin C) should be 500-1000 mg. The following foods are richest in this vitamin:
- Rosehip (1000 mg/100 g)
- Sweet pepper (250 mg/100g.)
- Sea buckthorn (200 mg/100g)
- Blackcurrant (200 mg/100g.)
- Kiwi (180 mg/100g)
- Brussels sprouts (100 mg/100g.)
Massage for bedsores
In the television program of the famous doctor Elena Malysheva, massage is considered as a means of preventing the occurrence of bedsores. This measure is also relevant for patients with existing injuries, since the presence of a lesion in one area leads to an even greater limitation of mobility and contributes to the development of new lesions of the skin and soft tissues. To stimulate blood circulation, it is recommended to rub the patient’s body daily with a hand in a special mitten on which camphor alcohol (10%) is applied.
The Protocol for the Management of Patients with Pressure Ulcers also considers massage as a preventative measure for the development of new lesions. However, it is indicated that massage cannot be performed in the area of bone protrusions; it is necessary to limit massage movements around these areas. Also, under no circumstances should massage be performed in areas where there are already violations of the integrity of the skin and underlying tissues.
Phonics is an effective method for treating bedsores
The effectiveness of using vibroacoustic therapy is associated with its ability to increase the overall microvibration background in the body. A patient forced to lead a sedentary lifestyle suffers from a severe deficiency of microvibration of muscle cells associated with lack of movement, which leads to disorders in all organs and tissues. Vibroacoustic therapy is a unique opportunity to saturate the body with the most valuable resource when there is a lack of movement.
What problems can be solved using Vitafon devices for patients with limited mobility?
- Improve blood circulation all areas of the body, including the skin and muscles in the area where bedsores develop. At the same time, metabolic processes in tissues are activated, cell nutrition and oxygen supply are improved, which reduces the risk of their death;
- Stimulate the processes of removal (disposal) of dead and damaged cells, which are the environment for the development of infection, from the necrosis zone. This reduces the risk of purulent complications and creates conditions for tissue renewal (regeneration) in the bedsore area;
- Remove poisons and toxins from the body, formed as a result of the death and disintegration of cells and pathogenic microbes, which has beneficial effect for the work of the whole organism;
- Activate general and local immunity by improving the functioning of the lymphatic system, which also reduces the likelihood of infectious complications in patients with bedsores;
- Increase the overall microvibration background of the body, which will have a beneficial effect on the course of the underlying disease, prevent further decrease in the volume of muscle tissue, and increase the overall tone of the body.
The optimal solution for a bedridden patient would be to use a vibroacoustic mattress (composed of ). The 8 vibraphones included in its composition provide a simultaneous impact on the area of bedsores and surrounding tissues. The device can operate in automatic mode for up to 14 hours, providing the body with continuous and dosed exposure - automatic activation occurs for 3 minutes every 24 minutes.
 Thus, in order to understand how to treat bedsores in bedridden patients at home, it is necessary to know the causes of the development of these injuries and understand the features of caring for patients with limited mobility.
Thus, in order to understand how to treat bedsores in bedridden patients at home, it is necessary to know the causes of the development of these injuries and understand the features of caring for patients with limited mobility.
The main task is to notice in time the first signs of the development of damage to the skin and underlying tissues and take the necessary measures to prevent further development of the process and the occurrence of dangerous complications. Stage 1 and 2 pressure ulcers are characterized by minimal tissue changes, which are quite easy to deal with. It is enough to carry out a number of activities, including:
- Proper care, which involves eliminating the causes of bedsores: regularly changing the patient’s position in bed, timely toileting of the skin, etc.
- The use of special means to help prevent the development of bedsores: mattresses, pillows, circles.
- Vibroacoustic therapy() for resource support of the body.
- Proper nutrition(sufficient amount of protein and vitamins)
- Regular massage.
- Local treatment is the use of drugs with antibacterial, healing properties, etc., as well as special dressings.
- Taking general medications, including (if necessary), antibiotics as prescribed by a doctor.
At the same time, treatment of grade 3 bedsores, in which there is muscle damage, as well as grade 4, affecting the deep layers of tissue down to the bone, while the patient is at home, can be quite difficult and not give the desired effect. This is associated with a high risk of infectious complications, including the development of sepsis (blood poisoning). In order to promptly detect danger and take the necessary measures, such a patient must be constantly under the supervision of a doctor.
Therefore, if the process has gone far, you should not think about how to treat deep bedsores at home, but you need to contact your doctor as soon as possible, who can decide whether to hospitalize the patient. The presence of extensive and deep wounds (stage 3-4) is often an indication for surgery: the surgeon removes dead areas of skin, muscles, bones, and fills the resulting defect with tissue (flaps of skin, connective tissue and muscles), which are taken from other parts of the patient’s body .
It is especially important to take timely measures when it comes to patients with damage to the nervous system, metabolic and vascular disorders. In such cases, complications can develop quite quickly. Therefore, if, despite treatment at home, healing does not occur and the process continues to progress, you need to seek help!
 How to cure bedsores at home? It will help to achieve a positive effect in the treatment of skin and soft tissue lesions in bedridden patients. vibroacoustic therapy. Application allows you to have a local effect on the affected area, preventing the aggravation of the process and the addition of infectious complications. Also, saturating the body with healing energy helps cleanse the body of dead cells, toxins and poisons, improves blood circulation and metabolic processes in tissues, strengthens the immune system and gives strength to fight both the underlying diseases and the changes underlying the development of bedsores.
How to cure bedsores at home? It will help to achieve a positive effect in the treatment of skin and soft tissue lesions in bedridden patients. vibroacoustic therapy. Application allows you to have a local effect on the affected area, preventing the aggravation of the process and the addition of infectious complications. Also, saturating the body with healing energy helps cleanse the body of dead cells, toxins and poisons, improves blood circulation and metabolic processes in tissues, strengthens the immune system and gives strength to fight both the underlying diseases and the changes underlying the development of bedsores.
List of used literature:
- Baskov A.V. Features of surgical treatment of bedsores of different localization / Research Institute of Neurosurgery named after. Academician N.N. Burdenko, M, 2002
- Dibirov M.D. Bedsores. Prevention and treatment / Medical Council, No. 5-6, 2013.
- Vorobiev A.A. Treatment of bedsores in spinal patients / Bulletin of the Volgograd Scientific Center of the Russian Academy of Medical Sciences. – 2007 – No. 2.
- Klimiashvili A.D. Prevention and treatment of bedsores / Russian Medical Journal. – 2004 – T. 12, No. 12.
- / “Doctor” No. 7 / 2014
- Patient management protocol. Bedsores. /Appendix to the order of the Ministry of Health of Russia dated April 17, 2002, No. 123.
- Fedorov V.A., Kovelenov A.Yu., Loginov G.N. and others / St. Petersburg: SpetsLit, 2012.
You can ask questions (below) on the topic of the article and we will try to answer them competently!
The topic of the article is the classification of bedsores, how to recognize the different stages of bedsores in time, what types and degrees of bedsores exist. This information will help you respond to danger in a timely manner and contact a specialist to properly solve the problem.
It can be difficult for relatives caring for a bedridden or sedentary patient to understand what kind of lesion we are talking about and what measures need to be taken. After all, a bedsore refers to both minor damage to the skin, which can be eliminated with proper care, and deep ulcers on the body that pose a threat to life.
Classification of bedsores
Causes and risk factors for the formation of bedsores
The main reason for the formation of bedsores is a person’s prolonged stay in a stationary position. Limitation of mobility may result various situations: injuries, diseases that limit mobility, severe exhaustion, mental illness, coma, etc. Damage to the skin, and then soft tissues, primarily occurs in “bulging” areas of the body, in which there is a very thin layer between the bone tissue and the skin layer of fiber (fat tissue) and muscle.
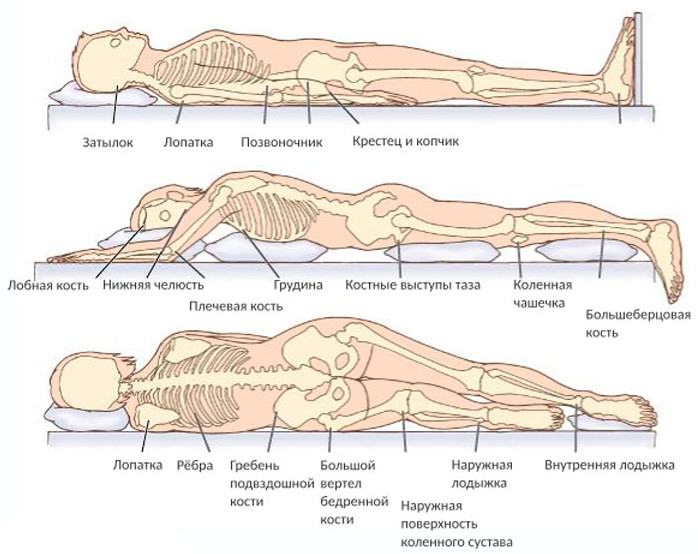
If the patient lies on his back, bedsores most often form in the area of the sacrum, coccyx, thoracic spine, heels, and less often in the back of the head and shoulder blades. In the prone position, the knees and the area of the iliac bones (protruding areas) are more often affected. pelvic bone), protruding surface of the chest. In the lateral decubitus position, tissues most often affected are the greater trochanter of the femur and the iliac crest. In sedentary patients, lesions often develop in the area of the closure of the buttocks, tailbone, and heels.
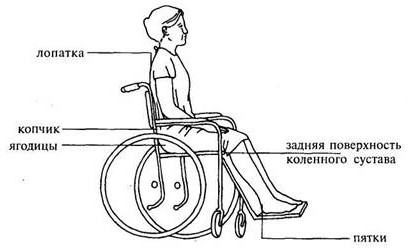
 How does a bedsore occur? In the area that is subject to pressure, blood circulation is impaired, causing cells to begin to suffer from a lack of oxygen and nutrients. Also, due to compression of the lymphatic vessels responsible for removing waste products from cells, waste and poisons begin to accumulate, poisoning the internal environment of the cell.
How does a bedsore occur? In the area that is subject to pressure, blood circulation is impaired, causing cells to begin to suffer from a lack of oxygen and nutrients. Also, due to compression of the lymphatic vessels responsible for removing waste products from cells, waste and poisons begin to accumulate, poisoning the internal environment of the cell.
In addition to pressure, factors such as friction, tissue displacement, and moisture play an important role in the development of damage to the skin and underlying soft tissues - you can read more about this. If the influence of the factors causing this entire cascade of damage does not stop, the cells begin to die - tissue necrosis (death) develops, spreading to the skin, subcutaneous fat and muscles.
The risk of developing pressure ulcers also depends on many other factors. Thus, in the Industry Standard " Patient management protocol. Bedsores", developed by the Ministry of Health of the Russian Federation, proposes a scoring system (Waterlow scale) for assessing the risk of developing pressure ulcers depending on age, gender, the presence of concomitant diseases in the patient, etc. The table below presents some of these criteria:
|
Criterion |
Indicators |
Risk level for developing bedsores (in points) |
|---|---|---|
|
Age (years) |
||
|
Food (features) |
||
|
Obesity |
||
|
Exhaustion |
||
|
Some diseases and bad habits |
||
|
Vascular diseases |
||
|
Anemia (anemia) |
||
|
Stroke, diseases and injuries of the brain and spinal cord, paralysis |
||
|
Incontinence |
Periodic diversion of urine through a catheter |
|
|
Fecal incontinence |
||
|
Fecal and urinary incontinence |
There are also types of pressure ulcers that occur as a result of pressure and friction from a cast (or other fixation material), vascular or urinary catheter. In addition, one of the most important reasons for the development of damage to the skin and soft tissues in sedentary patients is low level. The microvibration background of the body is created due to contractions of muscle cells, which are recorded not only during physical activity, but even at rest and sleep. This valuable resource is as important to sustaining life as air, water, food and heat. It is necessary for metabolic processes in cells and the directed movement of substances through blood and lymphatic vessels.
A sufficient level of microvibration is also needed for the full functioning of the lymphatic system, on which the condition of the body depends, the ability of the body to get rid of toxins, poisons (formed as a result of the vital activity of cells, the death of microbes, etc.), as well as. Maximum saturation of the body with microvibration energy occurs through physical activity - sports, walking, swimming, etc.
People who, for some reason, are deprived of the ability to move actively, and especially patients confined to a bed or wheelchair, develop a pronounced deficiency of microvibration energy in the body. What disorders that contribute to the development of bedsores does this lead to?
- The functioning of blood vessels suffers, which disrupts the delivery of nutrients and oxygen to tissues (including skin and muscle cells).
- Metabolic processes are disrupted in the cells, poisons and waste begin to actively accumulate, which accelerates cell death. Due to disruption of the lymphatic system and other organs (liver, kidneys) responsible for the processes of removing metabolic products from the body, which is also associated with a deficiency of microvibration, poisons and toxins accumulate. This leads to poisoning of the body, decreased organ function and the creation of a favorable environment for the development of pathogenic bacteria.
- Deterioration of the lymphatic system leads to decreased immunity, which also increases the risk of developing infectious complications.
Thus, a deficiency of microvibration accelerates the process of death of skin and muscle cells in patients, promotes the accumulation of dead cells, toxins and poisons in the body, increases the risk of infection: all this creates conditions for the development and progression of bedsores in bedridden patients.
The situation is aggravated by the fact that muscle cells, deprived of the ability to move, begin to decrease in size (atrophy), muscle mass becomes less and less, which leads to a further decrease in the level of microvibration in the body. In this situation, essential support for the body is - about its role in treatment And prevention of bedsores will be discussed further.
What are the stages of development of bedsores? In domestic and foreign medicine, there are different classifications, which are based on different criteria for assessing bedsores - external manifestations and symptoms, depth of tissue damage, cause of occurrence, presence of complications, etc.
The Protocol for the management of patients with pressure ulcers, a key document that all medical institutions in the Russian Federation are guided by, presents a classification that describes the symptoms of pressure ulcers at each stage. This classification is sometimes called dynamic. This definition implies that the dynamics of the process, that is, the transition from one phase to another, is not at all obligatory and immutable, but depends on many reasons and, above all, on proper care (especially in the initial stages). Also, timely resource support for the patient plays an important role - increasing the level of microvibration in the patient’s body.
According to the Protocol, there are 4 stages of pressure ulcers: below is a table that reflects this classification.
|
Stage of bedsore development |
Signs and symptoms |
|---|---|
|
The earliest stage in which the integrity of the skin is not compromised. What do bedsores look like in the initial stages? Visible on the skin at the point of pressure a focus of redness (hyperemia) that does not disappear after the pressure stops. As it increases oxygen starvation skin color changes. How do bedsores (stage 1) begin to look in the photo at this stage? It becomes noticeable that the area under pressure acquires a bluish tint and becomes swollen. The patient notes an increase in sensitivity in the area where the bedsore develops, which intensifies with pressure. Gradually, sensitivity decreases and numbness occurs, which is associated with pinching of nerve endings. |
|
|
Symptoms of this stage are associated with the death (necrosis) of skin cells and the upper layers of subcutaneous fat. First, the superficial layers of the skin (epidermis), and then the deeper ones (dermis), become thinner, and skin detachment occurs. Sign of second degree bedsores – formation of blisters at the site of pressure, peeling. A focus of inflammation may also be observed in the form of an elevation with a depression in the center (the beginning of the formation of an ulcer) |
|
|
Manifestations of this stage are caused by deep necrosis of the skin and subcutaneous fat with penetration into the muscles. The bedsore at this stage looks like wound or ulcer, there may be a discharge of clear or cloudy (purulent) fluid. |
|
|
The development of this stage is associated with the death of skin cells, subcutaneous tissue and muscles. Stage 4 bedsores look like a deep wound, at the bottom of which deep-lying tendons, joint elements, and bone tissue can be visible. |
 To better understand what bedsores look like, you can look at the photo: the initial stage is characterized by the presence of a focus of redness, the skin is not damaged, as oxygen deprivation increases, the skin acquires a bluish tint (the development of cyanosis)
To better understand what bedsores look like, you can look at the photo: the initial stage is characterized by the presence of a focus of redness, the skin is not damaged, as oxygen deprivation increases, the skin acquires a bluish tint (the development of cyanosis)
What do bedsores (stage 2) look like in photographs? Here we observe violations of the integrity of the skin - from peeling to the formation of a superficial wound.

In stage 3, the wound becomes deeper and muscle tissue may be visible. What do stage 4 bedsores look like? Views in photographs deep wounds, at the bottom of which bones, ligaments, and tendons may be visible.
Classification by stages of the pressure ulcer process
Professor M.D. Dibirov (Department of Surgical Diseases and Clinical Angiology of the A.I. Evdokimov Moscow State Medical University) also talks about the classification of pressure ulcers, focusing on the stage of the pressure ulcer process. In total, there are three stages: in order to understand what bedsores look like in each of them, you can look at the photos by stage.
Stage I – stage of circulatory disorders (vascular disorders)
This stage is characterized by changes caused by impaired blood circulation in the tissues. First, the skin becomes pale at the point of pressure, which is replaced by redness, then the skin acquires a bluish tint. What do bedsores look like in the initial stages? The photo shows areas of redness without clear boundaries, the integrity of the skin is not compromised.
Stage II – stage of necrotic changes and suppuration
At this stage, cell death (necrosis) occurs with damage to the skin and underlying tissues: fiber, muscles. At this stage, an infection may occur that affects both soft tissue (skin, subcutaneous tissue, muscles) and bone and joint tissue.
A bedsore at this stage may look like a superficial wound or a deep ulcer, in some cases having a dry surface and clear edges, in others there is purulent discharge and blurred edges, which indicates the spread of the process to the surrounding tissues.
Stage III – healing stage
At this stage, tissue regeneration (restoration) processes prevail in the area of the bedsore, the wound heals - the integrity of the skin is restored or a scar is formed.
Classification of bedsores by mechanism of occurrence
Also in medical practice, a classification is used, which is based on the division of pressure ulcers into groups, taking into account the mechanism of their occurrence. In this case, the role of the influence of external causes and internal disorders that play a role in the development of the damage we are talking about is taken into account
There are three types of pressure ulcers: exogenous, endogenous and mixed.
- Exogenous bedsores– damage, the occurrence of which is associated primarily with external influences (from the Greek exo - outside, genes - generated). First of all, we are talking about damage to the skin and underlying tissues that develop under the influence of factors that have already been mentioned above: pressure (as a key factor), friction, sliding, humidity. In turn, exogenous bedsores are divided into external and internal:
- External exogenous bedsores- these are the same injuries that develop from contact of the most protruding areas of the body (for example, the sacrum, shoulder blades, heels in the “supine” position) with a hard surface. This group also includes injuries resulting from pressure and friction of plaster casts (and other materials used for fixation in case of injuries), various corsets, poorly selected prostheses, etc.
- Internal exogenous bedsores – areas of damaged skin that appear as a result of constant pressure from catheters - tubes inserted into blood vessels to facilitate the administration of drugs, into the urinary canal or bladder for urine drainage. As a rule, they develop in patients with metabolic disorders, exhaustion, and problems with blood supply to tissues.
- Endogenous bedsores(from the Greek endo - inside) are associated primarily with internal violations in organism. Most often, such injuries occur in patients with lesions of the brain and/or spinal cord. This could be an injury, stroke (hemorrhage), tumor, etc. Such diseases lead to disruption of the nervous regulation of metabolic processes in tissues, disruption vascular tone. As a result, the nutrition of cells, including muscles and skin, suffers, which is the main reason for the development of damage. Such bedsores are often called neurotrophic ulcers (from the Greek trophe - nutrition).
The main danger of such lesions is that the death of muscle cells and the development of ulcers in muscle tissue often occurs when the skin is intact. Thus, it can be difficult to recognize and take adequate measures to treat them in time - ultrasound examination of soft tissues may be required to diagnose them. That is why patients with diseases and injuries of the nervous system need constant medical supervision.
- Mixed pressure ulcers develop when the body has internal problems (for example, exhaustion, cancer), as a result of which the regulation of tissue nutrition and metabolic processes suffers, and there are external influences - pressure, friction, etc.
 The tactics of their treatment depend on what factors (external or internal) are associated with the formation of bedsores. So, if external causes play a leading role, then the problem (especially in the early stages) can be solved with the help of proper care and well-chosen medications for local use.
The tactics of their treatment depend on what factors (external or internal) are associated with the formation of bedsores. So, if external causes play a leading role, then the problem (especially in the early stages) can be solved with the help of proper care and well-chosen medications for local use.
Why is it important to understand what causes damage? Because patient management tactics depend on this. If the problem is primarily related to diseases and injuries of the nervous system, metabolic disorders caused by various diseases, etc., then priority measures should be aimed at improving tissue nutrition, nerve conduction, normalizing metabolism, restoring blood supply to tissues, etc. If external causes play a leading role, then the problem can be solved (especially in the early stages) with the help proper care and well-chosen medications for local use.
At the same time, when we are talking about running processes (these are the third and fourth stages), then, for whatever reason, damage occurs, in order to eliminate them, in most cases it is necessary surgery. Besides, All patients suffering from bedsores are recommended vibroacoustic therapy, providing the body with a resource. In this case, the cause of the problem also does not matter.
Classification of bedsores by type of necrosis (cell death)
When, as a result of certain reasons, cells begin to die at the site of the development of a bedsore, an area of necrosis (dead tissue) appears. However, in different cases this process develops differently:
- Dry necrosis(mummification) is the “drying out” of the affected tissues. The lesion has clear boundaries, there is no discharge from the wound: infection occurs very rarely, in the initial stages, when a certain amount of fluid remains in the tissues. The patient may notice pain in the affected area, but the general condition most often does not suffer.
- Wet necrosis(bedsore gangrene) often develops in weakened patients with lesions of the nervous system, metabolic and vascular disorders. In this case, tissue necrosis occurs over large areas, and the damaged area often becomes infected. The wound is swollen, purulent discharge with an unpleasant odor is found in it.
As a rule, the development of pressure ulcer gangrene is accompanied by a sharp deterioration in the patient’s general condition: an increase in temperature, delirium, loss of consciousness, palpitations, and vomiting may be observed (as a consequence of poisoning of the body with microbial decay products). In the absence of adequate measures (prescription of antibiotics, surgical treatment), there is a high probability of developing sepsis - blood poisoning, often leading to the death of the patient.
Classification of pressure ulcers by size (diameter of lesion)
- Small bedsore: diameter less than 5 cm.
- Average bedsore: diameter is 5-10 cm.
- Large bedsore: diameter is up to 10 to 15 cm.
- Giant bedsore: diameter exceeds 15 cm.
It should be noted that a large diameter of a bedsore does not always indicate the presence of a severe process: extensive lesions can sometimes be superficial, occur without infectious complications and respond quite well to treatment without surgery. Of course, this picture is more common when it is not advanced bedsores that are observed, but the initial stage of the process.
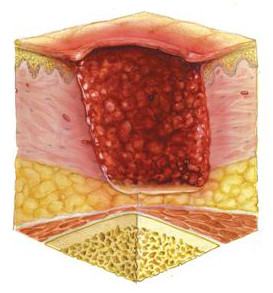 At the same time, an ulcer with a relatively small diameter can be quite deep, reach the muscle layer and serve as an entry gate for infection. A similar picture is often observed in patients with damage to the nervous system and blood vessels.
At the same time, an ulcer with a relatively small diameter can be quite deep, reach the muscle layer and serve as an entry gate for infection. A similar picture is often observed in patients with damage to the nervous system and blood vessels.
In this case, the so-called fistulous form of bedsore - the entrance hole (ulcer) in the area of the skin has a minimal diameter (less than 1 cm), it is a canal that leads into a deep cavity with purulent contents located underneath. Moreover, not only muscles, but also bone tissue can be involved in the inflammatory process with the development of osteomyelitis.
Classification of bedsore complications
Bedsores in patients are often complicated by the addition of an infectious process, especially when it comes to stages 3-4 (the presence of a deep ulcer with damage to muscle tissue). If the patient is in a hospital, there is a high probability of developing inflammation caused by a nosocomial infection, that is, pathogens that are resistant to the action of many antibiotics. When making a diagnosis in the case of complicated pressure ulcers, in addition to the stage of the process, the type of complication is indicated.
Depending on which tissues are involved in the inflammatory process, there are the following types infectious complications of bedsores:
- Phlegmon– inflammation of subcutaneous fatty tissue, connective tissue, which does not have clear boundaries. Most often caused by staphylococcus.
- Abscess- a focus of purulent melting of soft tissues (fiber, connective tissue, muscles) with the formation of a purulent cavity, which has clear boundaries.
- Osteomyelitis– melting of bone tissue. More often it occurs in areas such as the coccyx, sacrum, back of the head, and heel bones.
- Suppurative arthritis– inflammation in the joint area.
- Purulent melting of the vascular wall– can lead to both bleeding and the entry of purulent contents into the bloodstream.
- Sepsis– spread of infection throughout the body, in which case the formation of purulent foci may occur in various organs (heart, kidneys, lungs, joints, etc.) with the development of inflammatory processes in them. The entry into the blood of a large number of toxic (harmful) substances associated with mass death and the decay of cells, living and dead microbes and their metabolic products can very quickly cause the death of the patient.
It is also possible to develop complications such as erysipelas associated with the penetration of streptococci into the pressure wound. In some cases, in the presence of long-term non-healing ulcers, especially in patients with diseases of the nervous system and metabolic disorders, it is possible malignant degeneration (malignancy) and development of skin cancer at the site of a bedsore (Sh.M. Chyngyshpaev, 2013).
 Bedsores do not always develop in patients in the hospital. Often, relatives care for a patient with limited mobility at home. What should you do if you discover the damage that we are talking about in this article?
Bedsores do not always develop in patients in the hospital. Often, relatives care for a patient with limited mobility at home. What should you do if you discover the damage that we are talking about in this article?
First of all, it is necessary to call a doctor who can competently assess the condition of the skin and soft tissues at the site of development of the lesion and, if necessary, decide to send the patient to the hospital.
But this is not always necessary. For example, bedsores in which there is no deep tissue damage (as a rule, we are talking about the first and second stages) and there are no signs of an infectious process can be dealt with at home. In this case, the most important role is played by the organization of proper patient care, a rational diet and drinking regime, the formation of a favorable microclimate in the room where the patient is, the use of local medications, etc. You can read more about this in the article “ How to treat bedsores in bedridden patients at home?».
An effective means of treating and preventing bedsores is. Use in people with limited mobility helps to increase levels in the body and solve the following problems:
- Activation of metabolic processes in all organs and tissues, including skin and muscles.
- Improving blood supply to all tissues of the body.
- Stimulation of the process of removal (disposal) of dead cells, toxins and poisons due to improved functioning of the lymphatic system and other organs responsible for cleansing the body (kidneys, liver)
- Strengthening the immune system, thereby significantly reducing the risk of developing infectious complications.
List of used literature:
- Baskov A.V. Surgical treatment of bedsores in patients with spinal cord injury / Issues of neurosurgery - 2000 - No. 1
- Vorobiev A.A. Treatment of bedsores in spinal patients / Bulletin of the Volgograd Scientific Center of the Russian Academy of Medical Sciences - 2007 - No. 2
- Garkavi A.V. Complex treatment of bedsores in spinal patients. Dissertation of Candidate of Medical Sciences / Moscow, 1991.
- Dibirov M.D. Bedsores. Prevention and treatment / Medical Council, No. 5-6, 2013.
- Zilovich A. A. Surgical treatment of bedsores, trophic ulcers and osteomyelitis in patients with injuries of the spine and spinal cord. Dissertation of Candidate of Medical Sciences / Donetsk, 1986.
- Klimiashvili A.D. Prevention and treatment of bedsores / Russian Medical Journal – 2004 – T. 12, No. 12.
- Kogan O. G. Classification and combined conservative-surgical treatment of bedsores and bursitis in cases of spinal cord lesions. Guidelines for doctors / Novokuznetsk, 1976.
- / “Doctor” No. 7 / 2014
- Musalatov H.A. Treatment of bedsores in patients with damage to the spine and spinal cord / Medical Care - 2002 - No. 3.
- Patient management protocol. Bedsores /Appendix to the order of the Ministry of Health of Russia dated April 17, 2002. No. 123.
- Fedorov V.A., Kovelenov A.Yu., Loginov G.N. and others / St. Petersburg: SpetsLit, 2012.
You can ask questions (below) on the topic of the article and we will try to answer them competently!
A sick person who has been on bed rest for a long time constantly experiences discomfort - numbness in the limbs, pain, inability to go to the toilet on his own, depression. All this inevitably leads to a deterioration in the patient’s condition, and as a consequence, the development of the disease and the appearance of complications. Bedsores are the result of constant compression of skin and tissue. Most often, bedsores appear in bedridden patients.
The most reliable and effective method treatment - eliminate the cause of necrotic changes. If the patient can move independently, he needs to create a set of physical exercises for daily exercise. If a person is completely immobilized, a guardian must be present at all times and regularly perform hygiene procedures. In the initial stages, it is possible to quickly relieve the symptoms of necrosis and cure bedsores. In later stages, rapid treatment is not possible.

Symptoms
Depending on the degree of damage to the skin and soft tissues, experts distinguish 4 stages of the development of the disease. The appearance of bedsores can be determined by the following symptoms:
- pain and changes in skin color during palpation;
- swelling;
- tingling, burning and itching sensations;
- swelling and violation of the integrity of the skin;
- Sometimes bubbles form and can also be felt in a certain area.
The main symptoms of bedsores at the initial stage are a change in the color of the compressed areas of the skin and the appearance of compactions. Open wounds can not be. It is at this stage that bedsores can be quickly and completely healed.

The next stage is defined as transitional, since weeping wounds and ulcers form in places of compression, the integrity of the skin is damaged, bedsores increase in size and depth (necrosis of the subcutaneous tissue begins). For quick treatment, it is important to maintain cleanliness and order in the location of the bedridden patient, and promptly change and treat wounds. In the treatment of pressure wounds of the second stage, modern medications help well.
It is almost impossible to quickly cure stage 3 and 4 bedsores. This is due to the fact that not only the upper layer of the epidermis is affected, but also the muscles and tendons. Most often, the healing process is slowed down due to constant liquid discharge and deep infection of the wounds. Treatment of necrotic lesions at these stages should be entrusted to a specialist.

Bedsores are tissue changes of a dystrophic and ulcerative-necrotic nature. Bedsores appear on areas of the body that are subject to systematic pressure. They are also formed as a result of various neurotrophic disorders in patients who have been lying down for a long time. In such patients, a prolonged load is created on certain areas of the body, as a result of which a violation of tissue trophism is observed. In most cases, bedsores appear in the area of the coccyx, sacrum, and ischia. Much less often they form in the area of the hip joint, ribs, back of the head, and heels.
Bedsores are also dangerous because, with external minimum skin lesions they can cause intense damage to deeper tissues, often bones, in the structure of which deep cavities and pockets can form. This is often observed with bedsores that have formed in the area of the hip joint and/or sit bones. Long-term bedsores are often the reason for amputation of the joint (hip) and/or lower limb.
Bedsores can be complicated by inflammation of bone tissue in the form of osteomyelitis and periostitis. That is, if the bone is close to the bottom of the wound, then we are talking about contact osteomyelitis. At first, the discharge from this wound is almost transparent; later, when an infection occurs, purulent contents begin to form, sometimes with a putrid, fetid odor.
Causes of bedsores
Almost everyone knows that the tissues of the human body function when they receive the necessary nutrients through the bloodstream. Blood vessels, which permeate all human tissues in millions, appear as elastic tubes that are a kind of “conductor” of blood to all organs and tissues of the human body. The smallest of the blood vessels are called capillaries, which are extremely important for optimal metabolism in the body. The flow of blood through such tubes can be easily slowed down or stopped altogether by squeezing them. In every sitting or lying person, compression of the blood vessels begins to occur, and, as a result, compression of the soft tissues, the cause of which seems to be inadequate blood flow to the tissues. When this condition lasts more than two hours, ischemia begins to develop, and later necrosis of soft tissues. The bedsore begins to develop.
There are endogenous and exogenous bedsores in a patient. The factor of strong long-term compression of soft tissues plays a certain role in the cause of the development of exogenous pressure ulcers.
Internal and external exogenous bedsores are determined. External pressure ulcers often appear in places where there are virtually no muscle fibers between the skin under pressure and the underlying bone. For example, such places include: the back of the head, shoulder blades, femoral condyles, area olecranon, sacrum, etc. Typically, these bedsores are observed in patients after operations or after injuries, who are forced to remain in a certain position for a long time, usually lying down. The main causes of exogenous bedsores include: incorrectly fixed plaster splints or plaster casts, incorrectly fitted prostheses, medical orthopedic devices and corsets, as well as tight bandages, folds of clothing and sheets. Internal exogenous pressure ulcers develop under hard catheters or drainages that remain in the wound cavity or organ for a long time.
Endogenous bedsores appear with intense circulatory disorders and neurotrophic disorders. Endogenous mixed and neurotrophic pressure ulcers are determined. Mixed pressure ulcers are observed in weakened patients who cannot independently change the position of a limb or body. Prolonged immobility leads to ischemia of the skin, impaired microcirculation in the area of bone protrusions and the development of bedsores.
Endogenous neurotrophic pressure ulcers appear in patients with damage to the spinal cord, large nerves, stroke, or brain tumor. Due to disruption of innervation, persistent neurotrophic disorders begin to develop in tissues. For the development of neurotrophic pressure ulcers, the weight of one’s own skin over bone protrusions is sufficient. For example, above the costal arches, above the upper anterior iliac spines.
Risk factors for the development of bedsores in a patient are: poor nutrition and insufficient fluid intake into the body, or exhaustion, diseases of the cardiovascular system, urinary incontinence, injuries and back fractures, contaminated skin, crumbs and small objects under a bedridden patient, folds and seams on clothes.
Stages of bedsores
As mentioned above, bedsores form in those places that are subject to prolonged pressure for a long time and the blood supply in such places is disrupted. Bedsores are classified, as a rule, according to the depth of their damage to soft tissues; so to speak, assess the condition of the affected tissues and their depth.
There are 4 stages of development of bedsores:
— The first stage of bedsores is characterized by tissue compaction in the affected area and its hyperemia, swelling may be observed. At this stage, bedsores are very well treated with antibacterial therapy using wound-healing drugs.
— The second stage of bedsores is characterized by the formation of erosions and ulcers in the affected area. But, at this stage, proper tissue damage has not yet occurred. Only the upper layer of the epidermis is affected. The second stage can also be successfully treated, and with well-chosen and carried out tactics, a stable improvement in the condition of a patient with bedsores is possible.
— The third stage of bedsores is characterized by deeply intense damage to the tissues that are located under the skin. Damage to the subcutaneous layer occurs, which ultimately leads to irreversible necrotic lesions. This stage is extremely difficult to treat.
— The fourth stage is characterized by excessive damage and necrotic changes in soft tissue, as well as impaired circulation in these areas. Such changes can ultimately lead to severe intoxication of the entire body and further blood poisoning (sepsis).
Clinical manifestations of bedsores in a patient appear against the background of a main, often extremely serious disease and depend on the type of pathogenic microflora and the nature of necrosis. In the first stage, moderate local pain and a slight feeling of numbness are determined. In case of spinal cord injury, areas of necrosis can form within a day; in other cases, the transition of bedsores to the second stage of the process is slower.
With the development of bedsores in the form of dry necrosis, the patient’s condition does not change much, because the intoxication of the body is not very pronounced. The mummified lesion ends in a line of demarcation because dry necrosis does not spread.
A different clinical picture can be observed when bedsores appear in the form of wet necrosis. Foul-smelling contents are released from under necrotic tissues; as a result of the intensive proliferation of pathogenic and putrefactive flora, the purulent-necrotic process begins to rapidly spread. The resulting decubital gangrene provokes the development of purulent-resorptive fever and severe intoxication of the body. A rise in body temperature to 40˚C, delirium, depression of consciousness, chills, tachycardia, shallow breathing, decreased blood pressure, enlargement of the spleen and liver, etc. Severe intoxication is combined with proteinuria, pyuria, anemia and progressive dysproteinemia. In the blood there is a significant increase in leukocytes with neutrophilia with a shift to the left, and an increase in ESR.
Bedsores very often lead to complications. The most serious and common of these is sepsis.
Due to the fact that it is not always possible to determine only by appearance what specific stage of development the lesion of the skin and tissue is at, then for correct setting For diagnosis, they resort to methods such as the culture method and tissue biopsy from the pressure sore.
Bedsores treatment
Treatment of bedsores should be carried out based on two main conditions: rapid restoration of optimal blood flow to the damaged area of the body; necessary measures for the rapid healing of wound cavities that have formed as a result of bedsores.
When the color of the skin changes, stop all pressure on this skin area by changing the position of the body; the skin is treated with camphor alcohol; place an inflatable rubber circle under the patient; wash the patient with cold water. With the development of areas of necrosis, local therapy is aimed at drying necrotic tissues and preventing the transition of dry necrosis to wet necrosis. To do this, they resort to using: 1% potassium permanganate solution, 0.5% aqueous-alcoholic solution of Chlorhexidine, 1% brilliant green solution. The area of deep bedsores is covered with a dry antiseptic bandage. At this stage, the use of ointments and wet dressings. After the scab is rejected from the bedsore and its wound cavity is filled with granulations, ointment dressings are used or autodermoplasty is performed according to indications.
For deep bedsores that occur in the form of wet necrosis, the main goal of local therapy is to achieve rapid rejection of necrotic tissue. Proteolytic enzymes are considered the most effective in this regard, in particular immobilized proteases with prolonged action and hydrophilic ointments (Levomekol, Levosin, Dioksikol). It is acceptable to use bandages with hypertonic solution. If necessary, in some cases necrectomy is performed, the use of which significantly reduces the treatment time for bedsores.
For decubital gangrene and other purulent-necrotic complications, surgical treatment is recommended, opening of purulent leaks, phlegmons, etc. with further drainage and therapy in accordance with the method of treating purulent wounds. Apply different methods plastic closure of defects that formed on the skin after excision of necrotic tissue, and the erosive surface of a bedsore. To close the wound, local tissues are used (rotation plasty with a pedicled flap, s-shaped plasty, etc.) or autodermoplasty with a split skin flap. Skin grafting is also used for extensive granulating wounds during the final stage of local therapy. Antibacterial therapy must be carried out taking into account the sensitivity of pathogenic microflora to it.
In addition to local therapy, intensive high-quality treatment of the underlying disease, the use of stimulating and detoxification therapy should be carried out. To achieve this goal, blood transfusion is used; solutions of hemodez, rheopolyglucin, etc.; They use immunostimulants, vitamin therapy, and prescribe high-calorie diets.
Anti-exudative therapy is well achieved using Delaskin powder. Careful care of bedsores and the skin around them is considered very important. Several times a day, it is recommended to use local baths with Delaskin powder, which promotes healing and epithelization of bedsores. During hygienic procedures, wiping must be carried out with great care, avoiding strong friction against the patient’s skin. After hygienic procedures, the wound cavity is left until completely dry. It is also necessary to apply wet-dry compresses with Delaskin. They continue therapy for 5-7 days.
Antibacterial therapy begins a couple of days after the start of the main treatment. The use of Fusicutan cream is recommended. The cream is applied in a thin layer to the area affected by the bedsore 3 times. per day for 7 days.
For good healing of bedsores, the drug Vulnostimulin is used. It begins to be used on the 9th day after the start of the main therapy, 2 times a day in the morning and in the evening. Therapy continues until the bedsore is completely healed.
For deep bedsores, especially when the damaged area is extensive and difficult to heal, tissue transplantation is performed.
The prognosis for exogenous external pressure ulcers is usually favorable, because after eliminating pressure on the tissue and carrying out adequate therapy, a complete cure can be achieved very quickly. Exogenous internal pressure ulcers are considered more severe pressure ulcers for treatment due to the likelihood of damage to the walls of capillary vessels and hollow organs with the possibility of severe complications. With endogenous pressure ulcers, the prognosis is usually unfavorable, because the patient’s condition is significantly complicated by the underlying disease, and the occurrence of a purulent-necrotic process actually reduces the likelihood of a favorable outcome.
Bedsore treatment at home
Despite the fact that the formation of bedsores is a slow process, their treatment and prevention is still necessary. For treatment at home, it is recommended to apply a bandage to the affected area. This method is considered both a way to protect against pathogenic microorganisms and a way to better absorb the ointment into the affected area. A rectangular gauze bandage is applied to the skin and fixed with a hypoallergenic patch along its contour, holding onto healthy areas of the skin. It is better to apply the ointment to the center of the bandage, and not to the center of the bedsore. This therapy can help within two weeks.
Treatment of bedsores at home is recommended to be carried out already in the case of slight hyperemia of the skin and the first manifestations of a bedsore. Treatment is carried out with Tsindol emulsion or zinc ointment. The use of Menalind series cream is also recommended. It also contains zinc oxide. After applying the cream or ointment, the affected area is covered with a bandage. As a rule, the development of education stops.
If there is no skin on the damaged area and deep bedsores up to 2 cm in depth have formed, but there is no green, yellow, purple or red-black plaque and no purulent contents, it can be treated with this remedy. Take a container and wipe it with alcohol. Add part of Dioxidin 1% solution to three parts of Vishnevsky balm. Since these two drugs do not combine well, you need to mix everything thoroughly until it has a homogeneous consistency. For the treatment of bedsores, the prepared composition is applied for 2 days. After this period of time, healing usually begins and a new dressing with a new prepared composition is applied again. If you change the bandage every day, then there may be no effect from the treatment. In some cases, the use of Levomikol ointment is recommended. But according to the latest results of its use, this ointment gives a little noticeable therapeutic effect.
Treatment of bedsores at home is also carried out using medications in the form of Panthenol and Methyluracil ointments, but again, their effect is weaker.
In certain cases, bedsores are recommended to be treated with a thick solution of potassium permanganate. Although potassium permanganate does not help destroy microorganisms, the treated area quickly becomes covered with a crust of black necrotic tissue, under which pathogenic microflora can continue to develop. The purulent process spreads into the deeper layers of soft tissue and the inflammatory process can reach the bone. An unpleasant putrid odor may be heard from the wound cavity. This condition threatens the development of sepsis.
Often, bedsores are treated at home using a variety of methods. traditional methods and means, for example, cabbage leaves. But, as practice shows, in this case it is better not to use this method, since only a surgeon can provide assistance. He excises the necrotic crust from the dead tissue. Afterwards, the wound cavity must be treated with special preparations to remove necrotic tissue.
Treatment of bedsores
Initial care for pressure ulcers should be provided if the patient has redness and swelling at the sites where they appear. As a rule, these are the places where the patient lies for a long time. Later, the skin gradually peels off in thin films, gradually exposing deeper layers. The surface of the skin becomes moist, and pink fluid may be released.
If the pathological process is not stopped in time and its treatment is not started, in such good conditions for the proliferation of pathogenic microflora, numerous ulcers quickly begin to form on the skin, which can be covered with purulent plaque, forming deep bedsores.
As a rule, the patient does not complain of pain syndromes during this process. But this does not mean that the process stands still. Bedsores very often lead to irreversible processes of destruction of skin tissue.
If we do not take into account physiological factors, then the surface on which the patient lies plays a characteristic role in the rapid formation of a bedsore. For example, large folds in a sheet or a lumpy mattress can lead to the patient’s skin developing this disease much faster.
Constant treatment and care of bedsores can significantly speed up the recovery of patients.
The patient's bed should be as comfortable as possible for him. An exception may be the indication for a hard surface, for example, after a spinal fracture.
The bed linen of a bedridden patient should be smooth, dry and clean. It must be replaced every 2 days in order to prevent the development of pathogenic microorganisms from dirty laundry. The sheet should be well stretched and fixed on the bed, there should be no folds on it, and the hanging edges should be tucked under the mattress.
As necessary, special inflatable pillows or rubber circles are placed under the patient’s pelvic area.
During the day, the patient is periodically turned from one body position to another. When bedsores form, it is unacceptable for the patient to remain in one position for more than two hours.
Care and treatment of bedsores is a manual massage to improve blood circulation in those skin areas of the body that are constantly exposed to pressure.
Mandatory air baths are carried out. The affected skin areas are temporarily left uncovered for ventilation. This plays a special role in the care of bedsores.
Treatment of bedsores involves periodically replacing bandage and gauze dressings with medications. Medicines for treating bedsores can be in the form of ointments, creams and antiseptic solutions.
Ointment for bedsores
When a bedridden patient develops bedsores, the most effective method for treating them seems to be the use of ointments.
The main principles in the treatment of bedsores with ointments are: restoration of normal blood circulation to improve tissue trophism; stimulation and activation of general and local tissue regeneration processes; elimination and prevention of the development of bacterial infection in the wound cavity; elimination of possible pain and uncomfortable subjective sensations in the patient.
Accordingly, medications from different clinical groups, which are used in the form of ointments, can be used to treat bedsores. If absolutely necessary, certain of these same medications can be prescribed to the patient orally, that is, in the form of tablets or injections.
Treatment of bedsores should be carried out according to the stages and phases of the wound process, therefore, a specific complex is used for the treatment of each stage medicines.
During the first stage of the wound process, the so-called inflammation phase, medications are prescribed that help cleanse the wound cavity and inhibit the development of the infectious process. Also, these medications improve tissue trophism in and around the area affected by the bedsore. At this stage of the disease, the drugs Actovegin and Solcoserine can be used to improve blood circulation and accelerate tissue healing. At the beginning of therapy, concentrated 25% gels are used, and after two weeks they switch to using 5% cream. At the end of therapy, use 5% ointment until the end of the healing period. These two drugs are presented in the form of extracts from the blood of cattle, and if other experts dispute the advisability of using these drugs orally or injected, then modern medical practice for the treatment of bedsores considers these drugs to be irreplaceable and important component complex treatment.
Algofin ointment has also proven itself in the treatment of bedsores. It is also an extract from seaweed. Its action is based on its high chlorophyll content. It has a powerful antibacterial effect and activates the restoration of soft tissues.
In addition, ointments containing silver ions - Agrosulfan, Dermazin, Sulfargin - can be used to treat the first stage of bedsores. These medicines having antibacterial effect, significantly reduce the severity of burning and pain, accelerate tissue regeneration. Levomekol and Levosin ointments also have an antibacterial and regenerating effect, but their use for the treatment of bedsores at the first stage of a purulent-inflammatory process is not always advisable. If there is no evidence of microbial contamination of the wound cavity, then the prescription of medications that contain antibacterial substances can lead to the development of microflora resistance to the drugs used.
Vulnuzan ointment can also be used to treat the first stage of bedsores. This drug is good for cleansing the wound and sloughing off necrotic tissue. It also has antimicrobial and anti-inflammatory effects.
At the second stage of the wound process, or at the granulation stage, it is recommended to prescribe medications that have a drying effect. At this stage, ointments are prescribed that contain medicinal substances that stimulate the rejection of purulent masses and necrotic tissues, and also activate regeneration processes.
Betadine ointment, which contains iodine, is considered an effective drug. Due to iodine, the drug has an antimicrobial effect, destroys fungus that can enter the wound and promotes the development of viable granulations.
It is possible to use Methyluracil ointment, which contains provitamins that accelerate tissue regeneration and antimicrobial components. The drug has an immunostimulating effect, forms local immunity and promotes the death of pathogenic infectious agents without the development of resistance of these microorganisms to the treatment.
Thiotriazolin ointment stimulates recovery processes and local immunity. In addition, this drug, like Etonia ointment, has an anesthetic effect, eliminating discomfort in the wound cavity and in the tissues that surround it.
At the third stage of the wound process, or at the stage of epithelization, it is recommended to prescribe medications that accelerate the healing process. These medications include: ointments Bepanten, Curiosin, Mephenate, Alantan Plus. The choice of these medications explains not only the condition of the soft tissue in the area where the pressure sore appears, but also the principle of the development of the wound process. Naturally, together with the use of ointment in the treatment of bedsores, those drugs should be used that can help restore impaired physiological processes in the wound itself.
It should be remembered that due attention requires those wound cavities that are contaminated with a fungal infection, or those bedsores that occur in patients in a medical institution. In this case, it is necessary to use highly effective drugs, to whose antibacterial substances pathogenic pathogens of hospital infections have not yet developed resistance. In exceptional cases, the combined use of several medications is recommended, but with mandatory monitoring of their effect and the form of the wound process.
When treating bedsores, the use of medications that form an airtight film on the wound surface, including brilliant green solution, is strictly prohibited. Inadequate therapy can lead to an increase in the area of bedsores and a deterioration in the patient’s well-being.
Prevention of bedsores
To avoid the formation of bedsores, it is necessary to properly care for them and prevent them.
It is advisable to change bed linen every day. It is recommended to place a rubber circle on bedridden patients, who are especially forced to remain in this state for a long period of time in bed on their back. It is placed in a pillowcase so that the area of the sacrum is above its opening. If redness appears on the affected area of the skin, it is recommended to rub the skin in this area with a dry towel or quartz it. Such preventive procedures help improve local blood circulation in soft tissues.
You can also wash the affected skin with cool water and soap or wipe with an alcohol solution and then dust the skin.
good prophylactic agents When caring for bedsores, disinfectant and antiseptic solutions are used to wipe the skin. Such solutions include: camphor alcohol, which must be heated under running hot water before use; table vinegar and room temperature water are also good for preventing bedsores and disinfecting the affected area, which are used in equal parts and apply 2 tablespoons each. medical alcohol and cologne.
The patient's bedsores are treated according to a specific technique for wiping the skin. One edge of the towel is moistened with an antiseptic solution and lightly wrung out. They should wipe the area of the neck, back, behind the ears, chest area, and armpit area. Attention should also be paid to skin folds under the mammary glands, under which diaper rash may appear in sweating overweight women. After wiping with a damp towel, the skin must be wiped dry in the same order.
There are certain devices for preventing the formation of bedsores. These include: pads that are filled with gel, as a result of which their use distributes pressure over a larger area of the skin; a mattress filled with liquid distributes the patient’s body weight well, but such a mattress is very heavy. You can build it yourself by filling rubber gloves and bags with liquid and placing it under the affected areas of the patient’s body, or under those areas that require close attention: the back of the head, shoulder blades, buttocks, back of the calves, etc.
It is also convenient to use a mattress consisting of certain longitudinal sections to prevent bedsores. Their contents move depending on the direction of pressure applied to them. It is recommended to cover this mattress with one sheet to prevent the therapeutic effect from decreasing. But a cellular mattress, as a rule, consists of uneven and lumpy surfaces. Such raised areas on it, which consist of foam, provide preventive massage. And the indentations on such a mattress help relieve pressure on the patient’s skin. It is very convenient for use at home in wheelchairs, or on a bed.
All prevention of bedsores consists of careful care of the bedridden patient. It is recommended to ventilate both the room and the patient’s skin (air baths), because Bedsores really “love” moist skin areas. Adequate nutrition also contributes to the rapid recovery of the body after an injury or illness. And it should be remembered that their development often begins unnoticed. Therefore, prevention is considered a good preventative measure for the formation of bedsores.